Diabetic kidney disease (DKD) is the leading cause of chronic kidney disease (CKD) and end-stage kidney disease worldwide, affecting nearly 30–40% of patients with diabetes mellitus. The term DKD is broader than “diabetic nephropathy (DN)”: DN refers specifically to the classic histopathologic lesion complex attributable to diabetes on renal biopsy, whereas DKD includes any chronic kidney disease occurring in a diabetic patient, whether or not biopsy-proven classical diabetic lesions are present. This distinction is increasingly important because many diabetic patients have reduced eGFR without albuminuria, mixed lesions, or superimposed non-diabetic kidney disease (NDKD).
Clinical Presentation
DKD classically evolves through:
- Hyperfiltration phase (early increased GFR)
- Microalbuminuria (UACR 30–300 mg/g)
- Macroalbuminuria (>300 mg/g)
- Progressive GFR decline
- ESRD
However, modern phenotypes are heterogeneous:
A. Classical Albuminuric DKD
- Persistent albuminuria
- Progressive eGFR decline
- Often associated with diabetic retinopathy
B. Non-Albuminuric DKD
- Declining eGFR with normoalbuminuria
- More common in elderly T2DM, women, hypertensive patients
- Often associated with vascular/interstitial lesions rather than overt glomerulopathy
Clinical Clues Suggesting NDKD Rather than Pure DKD
- Sudden nephrotic syndrome
- Rapid creatinine rise
- Active urine sediment
- Absence of retinopathy
- Short diabetes duration (<5 years in T1DM)
Diabetic Nephropathy vs Diabetic Kidney Disease
| Feature | Diabetic Nephropathy (DN) | Diabetic Kidney Disease (DKD) |
| Definition | Histopathologic diagnosis | Clinical syndrome |
| Requires biopsy? | Yes | No |
| Scope | Classical diabetic lesions only | Includes all CKD in diabetes |
| May include NDKD? | No | Yes |
Thus, DN is a subset of DKD.
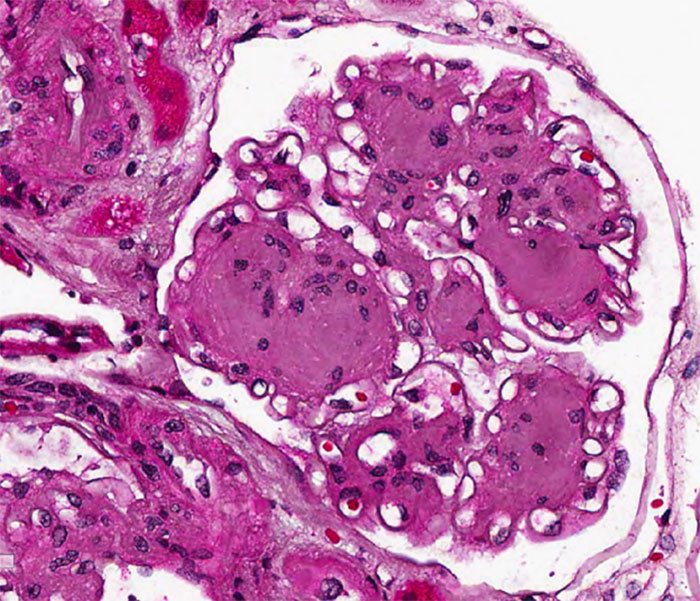
Histopathology of Diabetic Nephropathy
Renal biopsy is not routine but indicated when atypical features exist.
Classic Histologic Features (RPS Classification)
Glomerular Lesions:
- GBM thickening (earliest lesion)
- Diffuse mesangial expansion
- Nodular sclerosis (Kimmelstiel–Wilson nodules)
- Mesangiolysis
- Capillary microaneurysms
- Global glomerulosclerosis in advanced disease
Tubulointerstitial Lesions:
- Tubular basement membrane thickening
- Interstitial fibrosis/tubular atrophy (IFTA)
- Tubular atrophy
Vascular Lesions:
- Hyaline arteriolosclerosis (afferent + efferent arteriole hallmark)
- Arteriosclerosis
Patchy vs Diffuse Nature
A key diagnostic nuance: diabetic lesions may be patchy and heterogeneous, especially early in T2DM. Nodular lesions may involve only some glomeruli, while adjacent glomeruli may show only mild mesangial expansion. Hence biopsy sampling error can underestimate severity.
Emerging pathology studies using deep-learning morphometry show subtle early glomerular tuft contraction and peripheral capillary alterations even before overt nodular sclerosis develops.
Clinical Diagnosis of DKD
Diagnosis is usually clinical and based on:
Essential Criteria:
- Diabetes mellitus
- Persistent albuminuria (>3 months)
- Reduced eGFR (<60 ml/min/1.73 m²)
- Exclusion of alternate causes
Supporting Clues:
- Diabetic retinopathy
- Long-standing diabetes
- Bland urine sediment
- Gradual progression
Recommended Evaluation:
- UACR annually
- Serum creatinine/eGFR
- BP monitoring
- Retinal exam
- Potassium monitoring if RAAS blockade used
KDIGO recommends CKD staging using both eGFR and albuminuria grids.
Management: Current Evidence-Based Approach
A. Glycemic Optimization
- HbA1c target individualized: usually ~7%
- Avoid overt hypoglycemia in advanced CKD
B. RAAS Blockade
- ACE inhibitors / ARBs first-line in albuminuric DKD
- Reduce intraglomerular pressure and proteinuria
C. SGLT2 Inhibitors (Foundation Therapy)
Strong renal protective evidence:
- Empagliflozin
- Dapagliflozin
- Canagliflozin
Benefits:
- Slows eGFR decline
- Reduces albuminuria
- Lowers HF hospitalization
D. Nonsteroidal Mineralocorticoid Receptor Antagonist
Finerenone
- Proven benefit in persistent albuminuric DKD despite RAAS blockade
E. GLP-1 Receptor Agonists
Useful when:
- Additional glycemic control needed
- CV risk high
F. Blood Pressure Target
- Aim <130/80 mmHg if tolerated
G. Lipid Management
- Statins for cardiovascular protection
H. Dietary Measures
- Sodium <2 g/day
- Protein ~0.8 g/kg/day in non-dialysis CKD
I. When to Biopsy
Consider biopsy if:
- Hematuria
- Rapid renal decline
- Nephrotic syndrome
- No retinopathy + atypical course
Future Directions
Novel targets under study:
- Endothelin receptor antagonists
- Anti-inflammatory/fibrotic agents
- HIF pathway modulation
- Epigenetic therapeutics
Precision phenotyping may soon separate inflammatory, fibrotic, vascular, and metabolic DKD endotypes for individualized treatment.
References:
- Wang N, Zhang C. Recent Advances in the Management of Diabetic Kidney Disease. Int J Mol Sci. 2024.
- Correa-Rotter R et al. New and Emerging Therapies for DKD. Nat Rev Nephrol. 2024.
- Zhang H et al. Diabetic Kidney Disease: Current Evidence and Future Directions. Front Med. 2025.
- Mende C, Bloomgarden Z. Diabetic Kidney Disease Update. J Diabetes. 2025.
- KDIGO Diabetes in CKD Guideline Update Portal, 2026 draft update.

Dr Rashmi Shivram
Associate Consultant – Dept of Nephrology
Kauvery Hospital, Chennai.[1]

Dr Sanghamitra
Consultant Pathologist
Kauvery Hospital, Chennai.[1]

Dr. R. Balasubramaniyam
Chief Nephrologist
Kauvery Hospital, Chennai.[1]