Authors:
Dr. Avinash Sankar, MEM Second Year. Dr. Ashok, Consultant & Clinical Lead; Department of Emergency Medicine , Kauvery hospital alwarpet, Chennai
Abstract:
Background:
Post-stroke movement disorders (PSMDs) are uncommon, with an incidence of approximately 1–4% of all strokes. Among them, hemichorea–hemiballism is the most frequent in adults. Stroke presenting solely with abnormal movements, without motor weakness or sensory deficits, is exceptionally rare and may lead to diagnostic delay.
Case summary:
A 25-year-old previously healthy male presented to the Emergency Department (ED) with acuteonset, jerky, involuntary movements of the left upper and lower limbs since the previous night, worsening over four hours. He had a sudden-onset right-sided headache but no weakness, sensory loss, or speech disturbance. Neurological examination showed normal sensorimotor function with full power (5/5) in all limbs and isolated hemichorea involving the left upper and lower limbs. MRI brain demonstrated acute infarction in the right caudate and lentiform nuclei with focal tight stenosis of the right M1 segment. Serum homocysteine was markedly elevated (114.33 µmol/L). He was treated with intravenous sodium valproate, oral clonazepam, baclofen, and standard antiplatelet therapy. Movements subsided within 48 hours, and he was discharged on the second hospital day with complete resolution.
Conclusion:
Stroke presenting purely with abnormal movements is uncommon but clinically significant. Early neuroimaging is essential to prevent misdiagnosis. Elevated homocysteine represents a modifiable risk factor in young stroke patients.
Keywords:
Post-stroke movement disorder; hemichorea; hemiballism; basal ganglia infarct; hyperhomocysteinemia; young stroke; stroke mimic.
Introduction
Stroke is a leading cause of neurological disability worldwide. While motor weakness and speech impairment are typical presentations, movement disorders can occasionally be the first or sole manifestation of stroke, leading to diagnostic confusion.
Post-stroke movement disorders (PSMDs) occur in about 1–4% of stroke cases. In adults, hyperkinetic forms such as hemichorea–hemiballism predominate, whereas dystonia is more common in children. Lesions in the basal ganglia, thalamus, or their pathways are typically responsible. However, when stroke presents without weakness, as in this case, diagnosis may be delayed or mistaken for functional or metabolic causes.
We report a young male who presented with isolated hemichorea due to a right basal ganglia infarct secondary to hyperhomocysteinemia.
Case Report
Presentation
A 25-year-old male, with no comorbidities or prior medications, presented to the ED with involuntary movements of the left upper and lower limbs since the previous night. The movements were irregular, jerky, non-rhythmic, initially intermittent but continuous for four hours before presentation. They were aggravated by voluntary movement and had no relieving factors.
He also reported a sudden-onset right-sided dull aching headache at 10 pm the previous night. There was no limb weakness, numbness, speech difficulty, seizure, or altered sensorium. This presentation of isolated abnormal movement without focal neurological deficit posed a diagnostic challenge, with initial differentials including metabolic chorea, post-infectious chorea, and functional movement disorder.
Initial Assessment
- Airway: Patent
- Breathing: Bilateral air entry equal; SpO₂ 99% on room air; RR 20/min
- Circulation: BP 130/80 mmHg; PR 80 bpm; S1 S2 heard; no murmurs
- Disability: GCS 15/15; pupils 2 mm, equal and reactive
- Exposure: Temp 98.6°F; Capillary blood glucose 120 mg/dL
Arterial Blood Gas: pH 7.37, pCO₂ 42 mmHg, pO₂ 47 mmHg, HCO₃ 24.3 mmol/L
Serum Electrolytes: Na 136, K 3.6, Cl 105 mmol/L
Hb: 15.6 g/dL; Hct: 43%; Lactate: 2.2 mmol/L
Central Nervous System Examination
Higher Mental Functions: Conscious, alert, oriented
Cranial Nerves: Intact; no gaze palsy, facial weakness, or dysarthria
Motor System:
- Tone: Normal in all limbs
- Power: 5/5 in all muscle groups (Medical Research Council grading)
Involuntary Movements: Irregular, purposeless, jerky movements confined to the left upper and lower limbs, consistent with hemichorea. Movements increased with voluntary activity, absent during sleep.
- Reflexes: Normal; plantar response flexor bilaterally
Sensory System: Normal
FNT & FFNT – No dysmetria
Thus, the only neurological abnormality at presentation was unilateral choreiform movement without weakness or sensory deficit.
Investigations
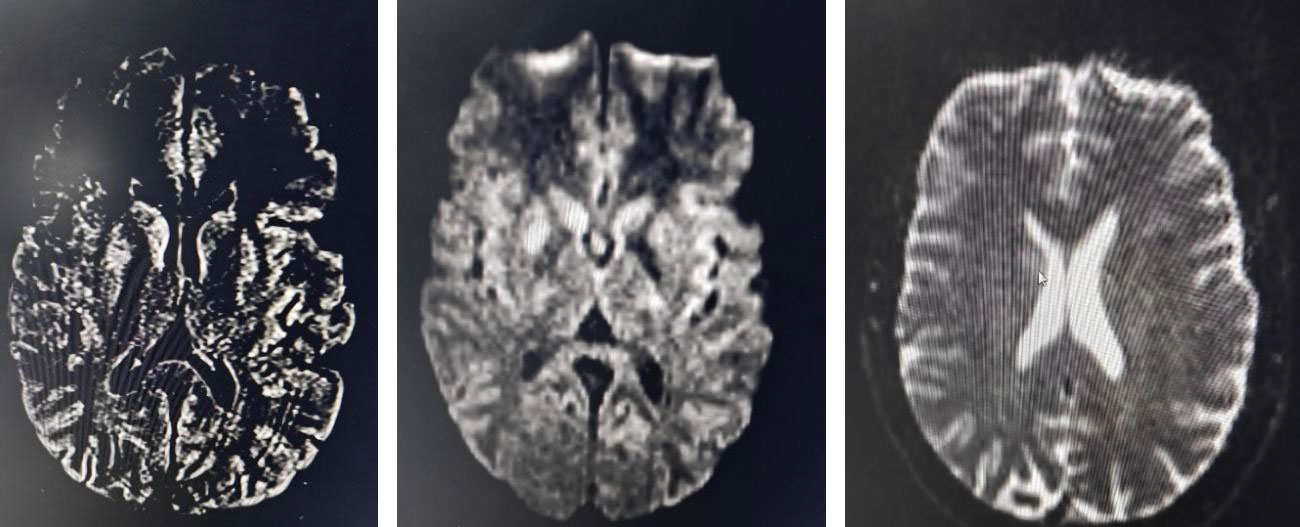
MRI brain (stroke fast protocol) revealed diffusion-weighted hyperintensity with corresponding low ADC values in the right caudate nucleus and lentiform nucleus, confirming an acute infarct
of the right basal ganglia.
FLAIR sequence demonstrated matching hyperintensity.
MRA showed a focal short-segment (2.3 mm) tight stenosis of the right M1 segment of the middle cerebral artery.
EEG was normal.
Serum homocysteine was markedly elevated (114.33 µmol/L). Other vascular risk markers were within normal limits.
Hospital Course
The patient was admitted under the Neurology team for evaluation and management.
He was initiated on:Inj. Sodium Valproate 1 g IV stat, followed by 1 g IV every 12 hours Tab. Rivotril (Clonazepam) 0.5 mg PO stat, Tab. Baclofen 10 mg PO stat, Tab. Ecosprin 300 mg PO stat, Tab. Tonact 40 mg PO stat

Over the next 24 hours, the intensity and frequency of involuntary movements decreased significantly. By 48 hours, movements had nearly become minimal and parientwas able to walk independently, with no new neurological deficits or recurrence.
He was discharged after 2 days of hospital stay with the following medications:
Tab Rivotril 0.5 mg – 1-0-1
Tab Clopitab-A – OD
Tab Revocon 25 mg – 1-0-1
Tab Modin 2.5 mg – 1-0-1
Tab Renerve Plus – 1-0-0
Tab Tonact 20 mg – 0-0-1
He was advised dietary modification, homocysteine correction, and neurology follow-up after 1 week.
Discussion
Stroke presenting as isolated hemichorea without weakness is rare and may easily be misdiagnosed or missed, particularly in young patients. Common differentials include functional movement disorder, metabolic causes (e.g., hyperglycemia, thyrotoxicosis), or drug-induced dyskinesia.
Pathophysiology
Lesions of the contralateral basal ganglia, especially the caudate and lentiform nuclei, interrupt inhibitory GABAergic pathways of the cortico-striato-thalamo-cortical loop, leading to
disinhibited thalamocortical drive and hyperkinetic movements.
In this case, the infarct in the right basal ganglia caused left-sided hemichorea without pyramidal or sensory signs, illustrating how small, localized vascular insults can produce isolated
movement disorders.
Diagnostic Importance
Such atypical presentations may be misinterpreted as benign chorea or functional disorder, delaying appropriate treatment. MRI stroke protocol imaging is crucial for early diagnosis, even
when focal deficits are absent.
Management
There are no standardized treatment guidelines for PSMDs. Symptomatic therapy with sodium valproate, clonazepam, or baclofen can effectively control movements. Vascular risk modification (antiplatelets, statins, and homocysteine correction) is essential for secondary prevention.
Most cases of acute post-stroke chorea resolve spontaneously within days to weeks. Our patient responded well to early therapy and metabolic correction, achieving complete resolution within
48 hours.
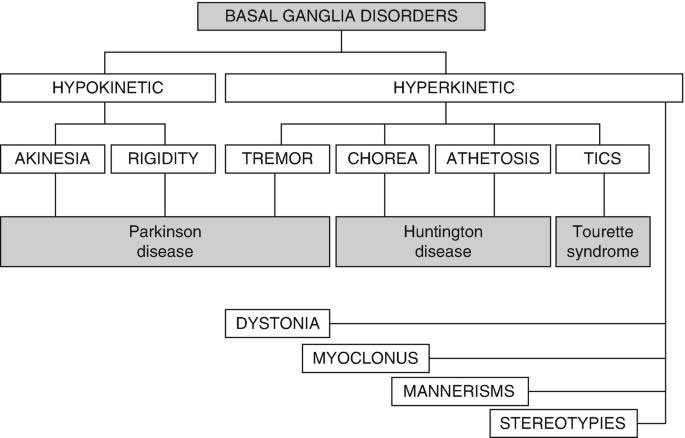
Types of Post-Stroke Movement Disorders Post-stroke movement disorders (PSMDs) are broadly classified into hyperkinetic and hypokinetic types.
-
- Hyperkinetic Disorders
- Chorea: Irregular, flowing, non-rhythmic movements involving distal limbs or face.
- Ballism: Violent, flinging, proximal limb movements (hemiballism).
- Athetosis: Slow, writhing movements of the hands and feet.
- Myoclonus: Sudden, brief, shock-like jerks of muscles.
- Tremor: Rhythmic oscillatory movement seen at rest or during action.
- Dystonia: Sustained contractions causing abnormal postures.
- Asterixis: “Negative myoclonus” causing flapping tremor on sustained posture.
- Hypokinetic Disorders
Vascular Parkinsonism: Bradykinesia, rigidity, and gait disturbance due to subcortical or basal ganglia lesions.
- Hyperkinetic Disorders
Clinical Significance:
Recognizing the type and timing of movement disorder provides clues to lesion localization. Early neuroimaging in such atypical cases can prevent missed strokes.
Conclusion
This case highlights a rare presentation of acute right basal ganglia infarction manifesting solely as left-sided hemichorea without weakness or sensory deficit.
Such atypical, purely hyperkinetic presentations may lead to misdiagnosis or delayed stroke recognition.
Prompt neuroimaging, metabolic work-up, and multidisciplinary management ensured early diagnosis and full recovery in our patient within 48 hours.
Clinicians should maintain a high index of suspicion for vascular causes in any new-onset unilateral movement disorder, even in young individuals.
References
-
-
- Tater P, Pandey S. Post-stroke Movement Disorders: Clinical Spectrum, Pathogenesis, and Management. Neurology India. 2021; 69(2): 272–283.
- Mehanna R, Jankovic J. Movement disorders in cerebrovascular disease. The Lancet Neurology. 2013; 12(9): 912–926.
- Siniscalchi A, et al. Post-stroke movement disorders: clinical manifestations and pharmacological management. J Neurol Neurosci. 2012.
- Handley A, Medcalf P, Hellier K, et al. Movement disorders after stroke. Age Ageing. 2009; 38(3): 260–266.
-

Dr Avinash
MEM Resident Emergency Medicine,
Kauvery Hospital, Alwarpet, Chennai.[1]