Renal disease presents a unique diagnostic challenge. Clinical manifestations such as proteinuria, hematuria, hypertension, or progressive renal insufficiency reflect functional disturbance but do not define the underlying structural pathology. Unlike many other organ systems, the kidney responds to diverse injuries with a limited repertoire of morphological patterns. The renal biopsy remains the gold standard for diagnosing medical renal diseases. A small core of renal cortex, when systematically processed and interpreted, provides detailed structural, immunologic, and prognostic information that directly influences therapeutic decisions.
The Scope of Nephropathology
Nephropathology encompasses a broad spectrum of disorders:
- Primary glomerular diseases
- Secondary involvement in systemic disorders (autoimmune, metabolic, infectious)
- Tubulo-interstitial diseases
- Vascular pathologies
- Hereditary nephropathies
- Renal transplant pathology
Many renal diseases share overlapping morphological patterns. Proliferative glomerulonephritis, for example, may result from immune complex deposition, complement dysregulation, or pauci-immune vasculitis, entities that differ fundamentally in pathogenesis and treatment. The role of the nephropathologist is to refine pattern recognition into etiologic classification.
Structured Evaluation of the Renal Biopsy
Renal biopsy interpretation is inherently compartment-based and systematic (figure 1).
Evaluation includes:
- Glomerular Compartment: Mesangial and endocapillary hypercellularity, basement membrane alterations, segmental versus global sclerosis, crescents and necrosis, and capillary thrombi
- Tubulointerstitial Compartment: Tubular atrophy and interstitial fibrosis strongly correlate with long-term renal outcome. Acute interstitial inflammation may suggest drug-related injury, infection, or immune-mediated disease.
- Vascular Compartment: Assessment includes hypertensive vascular changes, thrombotic microangiopathy, vasculitis, and transplant-associated vasculopathy. In certain cases, vascular findings are decisive for diagnosis.
Renal biopsy interpretation is therefore holistic rather than glomerulocentric.
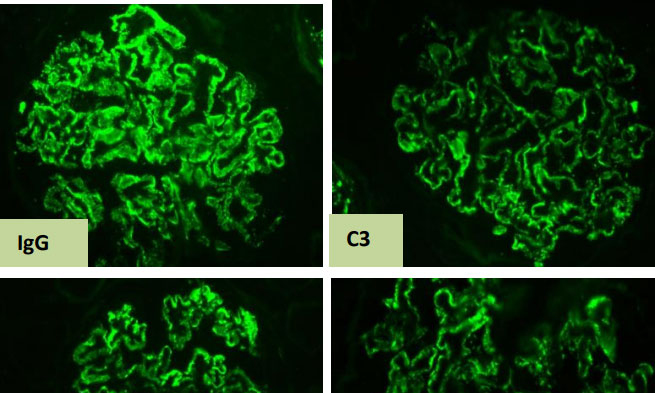
Immunofluorescence: Defining Immune Mechanisms (Figure 2)
Immunofluorescence (IF) is one of the most important tools in kidney biopsy evaluation. It helps us “see” immune proteins such as antibodies and complement deposited within the various compartments of a renal biopsy. By identifying what is deposited and where, IF helps us understand the mechanism of injury. DIF is helpful in diagnosing,
- Diseases caused by immune complex deposits
- Conditions driven mainly by complement activation
- Pauci-immune vasculitis, where little or no immune deposits are seen
- Disorders related to abnormal monoclonal immunoglobulins
In many cases, routine microscopy alone cannot provide the full answer. Immunofluorescence bridges that gap. The pattern of immune deposits transforms what may appear as descriptive structural changes under the microscope into a clear, mechanism-based diagnosis.
Electron Microscopy: The Ultrastructural Dimension
Electron microscopy (EM) provides ultrastructural detail that is critical in selected settings. Certain diagnoses including minimal change disease, early membranous nephropathy, hereditary basement membrane disorders, and some complement-mediated diseases may require EM for definitive classification. Thus, ultrastructural examination completes the triad of modern nephropathologic assessment. EM allows evaluation of:
- Podocyte foot process effacement
- Subepithelial, subendothelial, or mesangial electron-dense deposits in immunecomplex mediated injury
- Basement membrane thinning, splitting, or lamellation
- Organized deposits (fibrillary or microtubular structures)
Immunohistochemistry and Ancillary Techniques
Immunohistochemistry (IHC) further enhances diagnostic specificity. Selected markers assist in:
- Differentiating primary from secondary forms of disease eg: Membranous glomerulonephritis
- Identifying viral nephropathies in transplant recipients
- Detecting antibody-mediated rejection
- Supporting amyloid subtyping
Dedicated Nephropathology Services:
With the rising burden of kidney diseases, accurate and timely diagnosis through comprehensive kidney biopsy evaluation is essential for effective patient care. We are happy to share that a dedicated Nephropathology Unit has recently been started at our institution, Kauvery hospital, Alwarpet, Chennai.
References
- Jennette JC, Olson JL, Silva FG, D’Agati Heptinstall’s Pathology of the Kidney. 7th ed. Philadelphia: Wolters Kluwer; 2015.
- Fogo Approach to renal biopsy interpretation. Kidney Int. 2015;87:45–56.
- Haas M, Sis B, Racusen LC, et Banff 2017 update on renal allograft pathology.
Kidney Int. 2018;94:25–41. - Sethi S, Fervenza Pathology of glomerular diseases. Clin J Am Soc Nephrol. 2019;14:288–302.
Figure 1: Renal compartments evaluated on routine Light microscopic examination
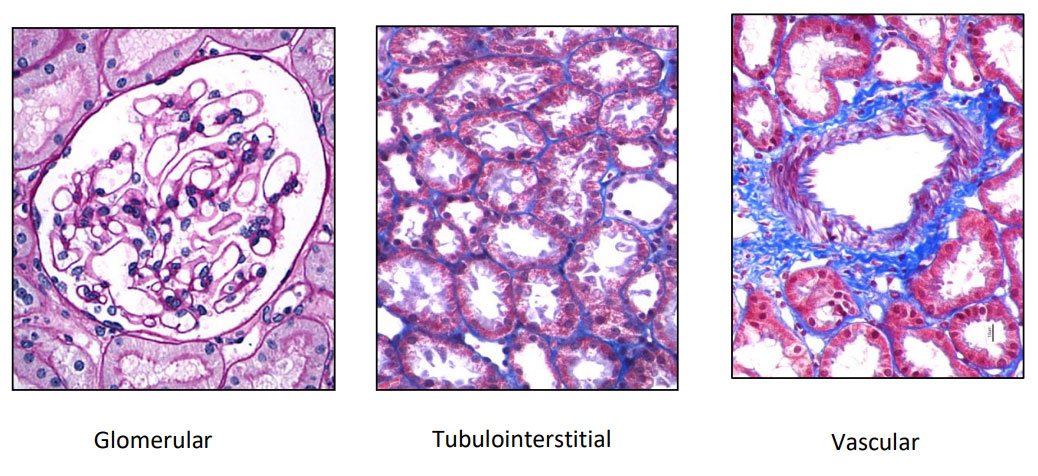
Figure 2: Immunofluorescence image illustrating 3+ granular deposits of IgG, C3, Kappa, and Lambda along the glomerular basement membrane in a case of Membranous glomerulonephritis

R Sangamitra MD, PDCC (Renal and Transplant Pathology)
Associate Consultant
Kauvery Hospital, Alwarpet, Chennai.[1]

Dr Priya Subash Chandra Bose MD, DNB, DipRCPath
Senior Consultant
Kauvery Hospital, Alwarpet, Chennai.[1]

Dr Sharon Milton, MD, DNB,
Consultant
Kauvery Hospital, Alwarpet, Chennai.[1]