Case Summary
Mrs. X, a 33-year-old woman, developed systemic hypertension and proteinuria during the third trimester of her pregnancy in 2014. She delivered preterm via LSCS and continued to have elevated creatinine (2.0 mg/dL). Renal biopsy revealed mesangial proliferative glomerulonephritis with chronicity.
In 2021, following a COVID-19 infection, her renal function worsened (creatinine 12 mg/dL), and she was started on maintenance hemodialysis. She underwent ABO-incompatible renal transplant in February 2024 with her mother as the donor. The perioperative period was uneventful, and she maintained good graft function.
Six months later, she presented with lower limb weakness and difficulty walking. Imaging showed multiple expansile lytic lesions. Biopsy confirmed brown tumors, and biochemistry revealed elevated PTH, hypophosphatemia, and vitamin D deficiency, pointing toward tertiary hyperparathyroidism.
Diagnosis
- Multiple Brown Tumors
- Tertiary Hyperparathyroidism
- Post-Renal Transplant CKD with Good Graft Function
Discussion
Tertiary hyperparathyroidism (3°HPT) is a relatively rare but clinically important complication following renal transplantation. It results from prolonged stimulation of the parathyroid glands during chronic kidney disease (secondary HPT), eventually leading to autonomous and unregulated PTH secretion even after successful kidney transplantation. This loss of feedback control occurs due to nodular or diffuse hyperplasia of the parathyroid tissue and is more likely in patients with a high pre-transplant PTH level and a longer dialysis vintage.
In a normal physiological state, declining serum calcium or rising phosphate stimulates parathyroid hormone secretion, which acts on the bones, kidneys, and intestines to restore mineral balance. After renal transplant, improved renal function should restore phosphate excretion and 1,25-dihydroxy vitamin D production, eventually normalizing calcium-phosphate homeostasis and suppressing PTH levels. However, in some patients, this regulatory mechanism fails due to pre-existing parathyroid autonomy—manifesting as tertiary hyperparathyroidism.
Our patient presented with brown tumors, one of the rare skeletal manifestations of prolonged HPT. These lesions are the result of rapid osteoclastic bone resorption driven by elevated PTH, causing marrow fibrosis and local hemorrhage, followed by deposition of fibrous tissue and hemosiderin. Though benign, brown tumors can cause significant morbidity due to bone pain, deformity, or even pathological fractures. Commonly affected sites include the pelvis, mandible, ribs, clavicle, and long bones.
The diagnosis in such cases rests on a combination of imaging, histopathology, and laboratory evidence. Radiographs or CT/MRI typically show well-defined lytic lesions, and biopsy reveals osteoclast-like multinucleated giant cells within fibrous stroma and hemosiderin-laden macrophages. Biochemically, these patients often exhibit normal or elevated calcium, low phosphorus, low vitamin D levels, and persistently high PTH values—despite restored kidney function.
This patient’s persistently high PTH and subsequent skeletal complications underscore the importance of routine monitoring and early intervention in post-transplant mineral bone disease. Although vitamin D supplementation and phosphate management are foundational, surgical treatment becomes necessary when medical management fails or complications such as brown tumors arise.
Parathyroidectomy remains the definitive therapy for tertiary HPT. The choice between subtotal resection and total parathyroidectomy with autotransplantation must consider recurrence risk. Studies, such as that by Triponez et al., suggest lower recurrence with total parathyroidectomy and autotransplantation. In most reported cases, brown tumors regress within 2–6 months of surgery, with notable improvement in bone pain and mobility.
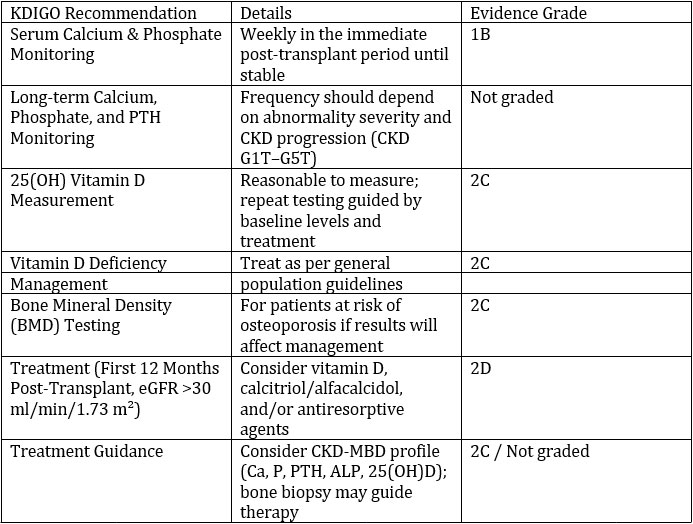
KDIGO Guidelines for Post-Transplant Mineral and Bone Disease
Indications for parathyroidectomy include:
- Persistent hypercalcemia (>10.2 mg/dL beyond 3–12 months)
- Brown tumors or osteopenia
- Bone pain, fatigue, pruritus, or pathological fractures
- Enlarged parathyroid glands (>1 cm or volume >500 mm³)
- Vascular, valvular, or soft tissue calcification
Surgical success is usually associated with rapid improvement in symptoms and biochemical correction. In our case, surgery was indicated due to brown tumors and persistently elevated PTH.
Conclusion
This case illustrates the critical importance of continued surveillance for CKD-mineral bone disorder (CKD-MBD) even after successful kidney transplantation. While transplant improves many metabolic parameters, not all complications resolve automatically. Persistent hyperparathyroidism and its skeletal consequences, such as brown tumors, demand vigilance and timely management. Early treatment can prevent irreversible bone damage and improve outcomes in post-transplant patients.

Dr Yashila
Nephrology PG Resident,
Kauvery Hospital[1], Chennai
Mentor

Dr Balaji Kirushnan
Consultant Nephrologist,
Kauvery Hospital[1], Chennai