CASE REPORT:
A 11 months old male baby who is a known case of Pierre Robin Syndrome (sequence) underwent Supraglottoplasty with glossopexy (Tongue lip adhesion)at 50 days of life for persistent respiratory distress as he had posterior fallback of tongue with supraglottic inspiratory collapse (Type II laryngomalacia). Currently posted for Tongue lip adhesion release.
General examination:
Active baby, normal developmental milestone, Immunized till date, Stable vitals.
Airway assessment:
Retrognathia, tongue-lip adhesion, anticipated difficult airways.

Investigation:
Hb-10.6g/dl TC-10,410/cu.mm INR-1.04
Echo-Good Biventricular systolic function, No PAH
Anaesthesia concern – Paediatric age group, Anticipated difficult intubation, needs video laryngoscope and the difficult airway cart should be ready.
PRE-OPERATIVE PREPARATION:
- The anaesthesia plan (General anaesthesia with Endotracheal intubation)and its associated complications were thoroughly discussed with the operating surgeon and clearly communicated to the patient’s representative. Informed and written consent was subsequently obtained.
- Nil per oral status was verified and adequate.
- Premedication included single dose of INJ PANTOPRAZOLE 10mg IV and INJ ONDANSETRON 1mg IV given. IVF DNS /RL was started at the rate of 40ml/hr.
- All essential resuscitation equipments were prepared and made readily available.
INTRA-OPERATIVE PLAN/MANAGEMENT:
- Standard ASA monitors were attached and vital parameters were observed continuously throughout the procedure.
- After preoxygenation with 100% Oxygen for 3minutes, with inhalational anaesthetic (Sevoflurane 2%) 22G Intravenous cannula was placed. INJ GLYCOPYROLATE 0.1mg I.V ,INJ FENTANYL 20mcg I.V,INJ PROPOFOL 20mg I.V,INJ ATRACURIUM 5mg I.V were given during induction. Endotracheal tube of size 4mm was secured with the help of video laryngoscope along with bougie. FREMANTLE score-P-2 -ProVu 1size blade Throat pack was placed.
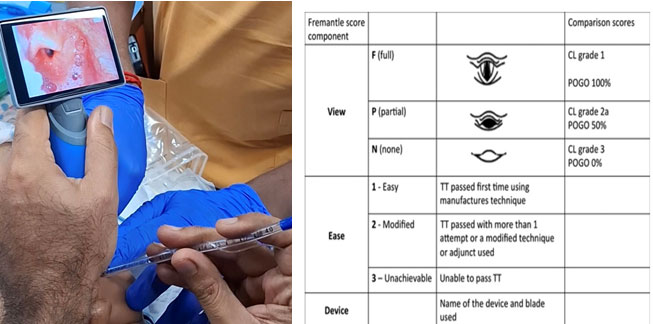
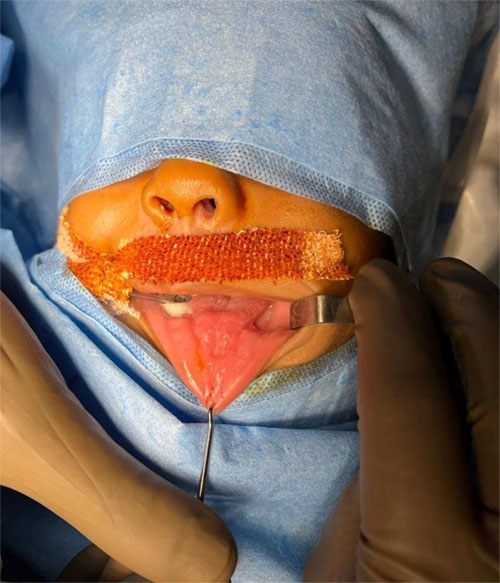
( Pre-Surgery picture)
- The patient was placed on mechanical ventilation [ pressure control mode -FiO2 48% Pinsp-22cmH2O, RR-26/min. Maintenance by inhalational anaesthesia (Sevoflurane 2%) along with oxygen and nitrous oxide.
- Throat pack was removed before extubation. INJ NEOSTIGMINE 0.5mg given as neuromuscular blocker reversal along with anticholinergic INJ GLYCOPYROLATE 0.1mg .Extubated after good spontaneous breathing efforts. Patient was hemodynamically stable throughout the surgery. Shifted to Post Anesthesia care unit for observation.
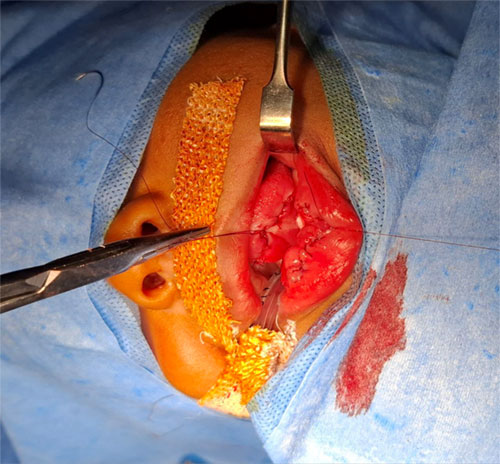
(Post-Surgery picture)
DISCUSSION:
Pierre Robin Sequence is characterized by a triad – Micrognathia, upper airway obstruction, glossoptosis. It affects approximately 1 in 14,000 newborns annually. At birth, affected infants often show signs of respiratory distress such as stridor, retractions, and cyanosis and may also struggle with feeding issues, gastroesophageal reflux, poor weight gain (failure to thrive), aspiration.
In around 70% of cases of Pierre Robin Sequence, placing the newborn in a prone/lateral position can effectively relieve airway obstruction. If the infant continues to desaturate, a nasopharyngeal tube may be used to bypass the upper airway. Infants with mild obstruction who are managed conservatively may still face challenges such as feeding difficulties, gastroesophageal reflux and aspiration, which can lead to failure to thrive. In these cases, inserting a gastrostomy tube can support adequate nutrition and promote catch-up growth, helping to prevent these complications. In situations of severe, acute airway obstruction, an emergency tracheostomy is required to secure the airway. After initial stabilization, surgical procedures like tongue-lip adhesion or mandibular distraction osteogenesis can be considered to correct tongue fall.
ANAESTHESIA CONCERNS:
- Airway management in patients with Pierre Robin Sequence presents considerable challenges due to underlying craniofacial anomalies. Facial deformities commonly impede the establishment of an effective seal for facemask ventilation. Direct laryngoscopy and tracheal intubation are typically difficult in infancy, although these procedures often become more feasible with age and mandibular growth.
- Postoperative airway collapse is a recognized risk in PRS patients. This may be precipitated by pre-existing upper airway obstruction, obstructive sleep apnea (OSA), chronic hypoxia and increased opioid sensitivity. Clinical indicators of respiratory compromise include paradoxical breathing patterns, sternal recession and tracheal tugging.
- Neonates with Pierre Robin Sequence exhibit heightened sensitivity to opioids, particularly those with OSA secondary to glossoptosis. This sensitivity is thought to result from upregulation of opioid receptors within the brainstem. Neonates with severe airway obstruction often require significantly reduced opioid dosages, necessitating cautious titration and vigilant monitoring in the perioperative period.
- Feeding difficulties are common in PRS and are often compounded by swallowing disorders and gastroesophageal reflux. These complications increase the risk of bronchial microaspiration and recurrent pulmonary infections. Accordingly, aspiration precautions are essential prior to elective procedures.
- Nutritional compromise is also prevalent in this population. Persistent feeding and airway difficulties contribute to malnutrition and a high incidence of failure to thrive, underscoring the need for multidisciplinary management.
References:
- Text book Miller’s Anesthesia 10th edition
- Frawley G, Espenell A, Howe P, Shand J, Heggie A. Anesthetic implications of infants with mandibular hypoplasia treated with mandibular distraction osteogenesis. Paediatr Anaesth. 2013 Apr;23(4):342-8.
- Airway management for intubation in newborns with Pierre Robin sequence. Alexander P Marston et al. Laryngoscope. 2012

Dr Mohamed Najibullah
Consultant Anaesthesiologist
Department of Anaesthesiology
Kauvery Hospital, Chennai

Dr Moushiga Subhashini
II Year DNB Resident
Department of Anaesthesiology
Kauvery Hospital, Chennai