Introduction
Acute mesenteric ischemia (AMI) is a life-threatening vascular emergency caused by abrupt compromise of intestinal perfusion, often associated with high morbidity and mortality. Early diagnosis is crucial to prevent irreversible bowel infarction. Contrast-enhanced CT angiography (CTA) is the imaging modality of choice for rapid and comprehensive evaluation of mesenteric vasculature and bowel viability.
While embolic and thrombotic occlusions of the superior mesenteric artery (SMA) are the most common causes of AMI, vasculitides such as Takayasu arteritis rarely involve mesenteric vessels. Inflammatory arterial involvement may predispose to luminal narrowing and thrombosis, leading to bowel ischemia.
We present a case of acute mesenteric ischemia in a patient with known aorto-arteritis, demonstrating inflammatory involvement of the superior mesenteric artery with distal branch thrombosis and advanced ischemic bowel changes on CT angiography.
Case Presentation
A patient with known aorto-arteritis presented with persistent upper abdominal pain associated with nausea. There was no history of vomiting, fever, or diarrhoea.
On examination, epigastric and periumbilical tenderness with guarding and sluggish bowel sounds were noted. Given the suspicion of vascular pathology, multidetector CT angiography was performed.
Imaging Findings
Vascular Findings
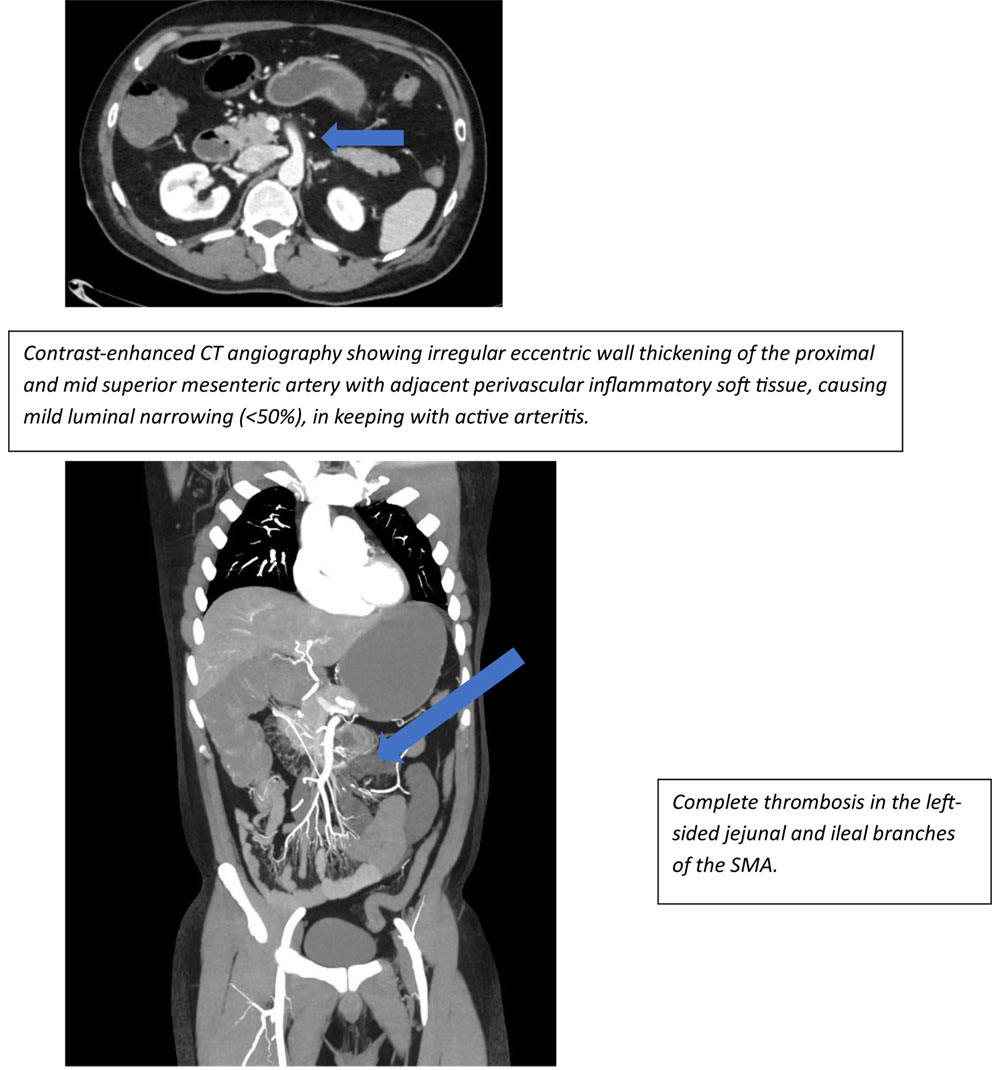
The proximal and mid segments of the superior mesenteric artery demonstrated irregular eccentric wall thickening with surrounding inflammatory soft tissue, causing mild luminal narrowing (<50%), consistent with active arteritis.
Complete thrombosis was noted in the left-sided jejunal and ileal branches of the SMA. Partial thrombosis was also seen in the right-sided ileocolic branches, associated with perivascular inflammatory changes.
Other major abdominal vessels, including the celiac axis and inferior mesenteric artery, were unremarkable.
Bowel Findings
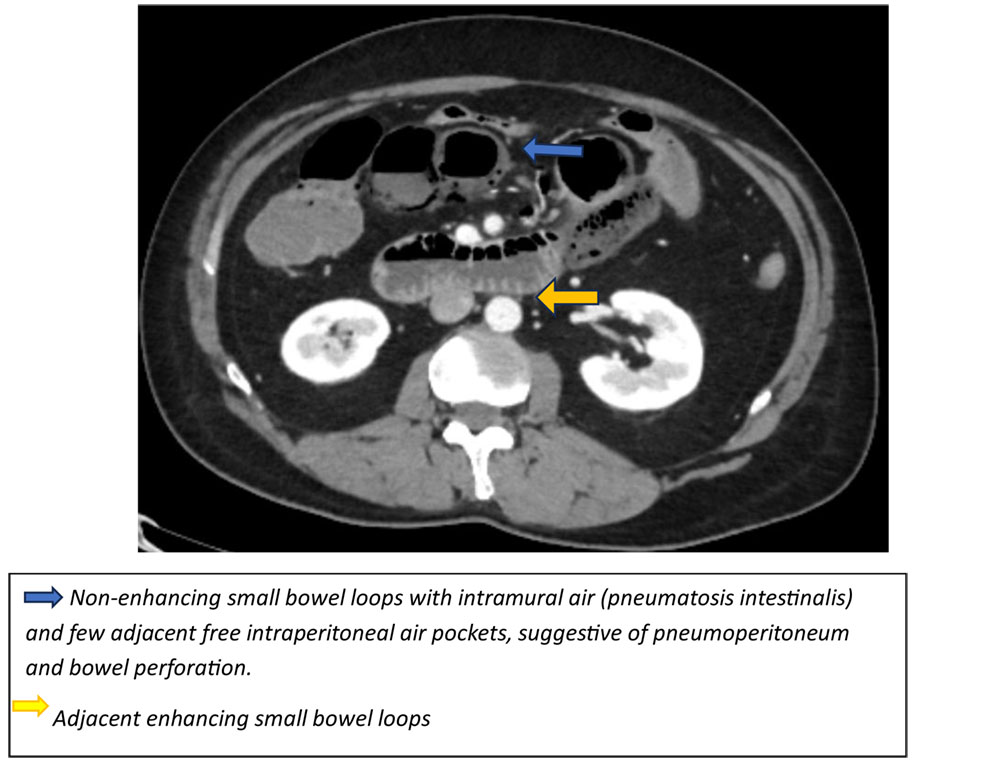
Multiple jejunal and proximal ileal loops were markedly distended and demonstrated:
- Marked bowel wall thinning
- Absent mural enhancement
- Pneumatosis intestinalis
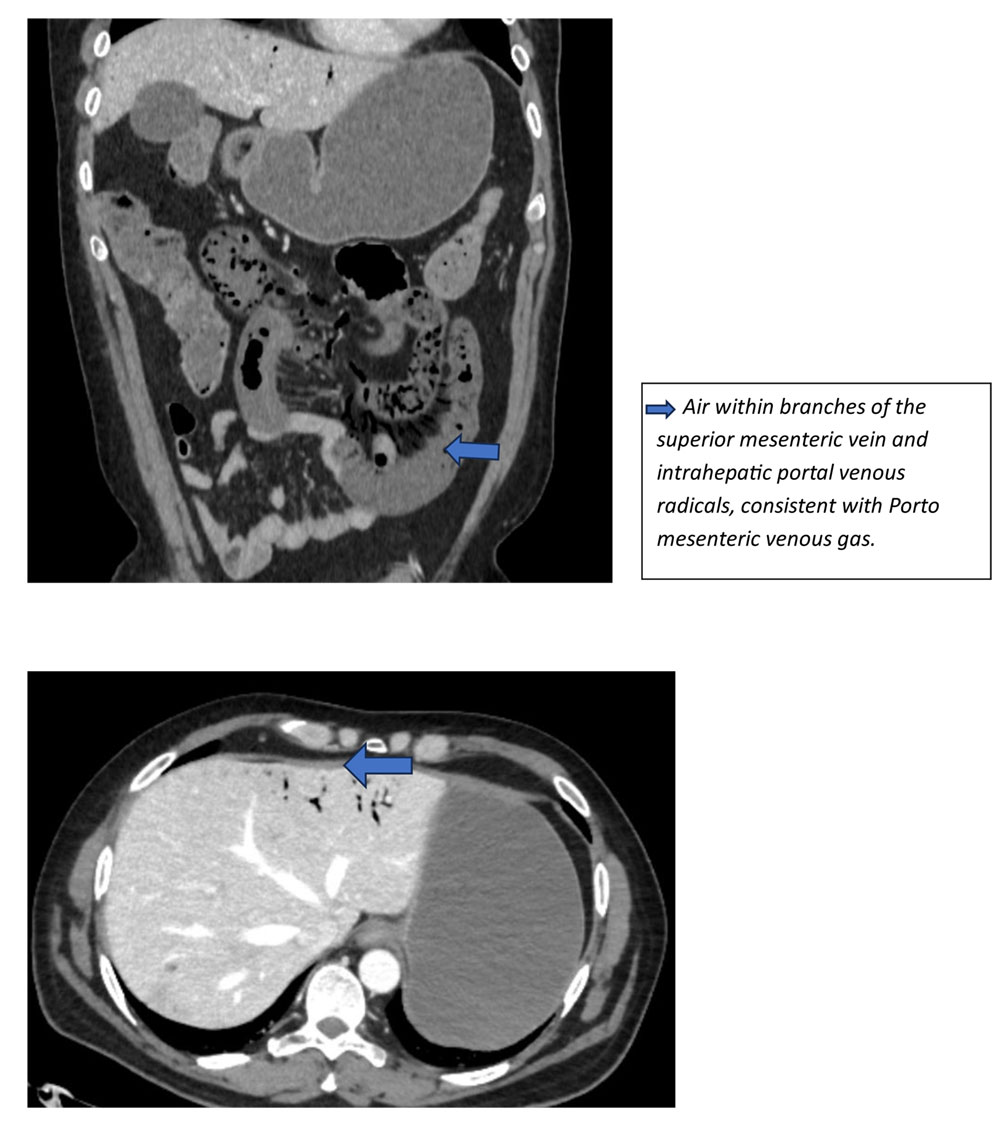
Air was noted within branches of the superior mesenteric vein and intrahepatic portal venous radicals, consistent with Porto mesenteric venous gas.
These findings are indicative of advanced bowel ischemia with likely transmural infarction.
Clinical Significance
Acute mesenteric ischemia requires rapid diagnosis and urgent intervention to reduce mortality. In patients with underlying vasculitis, inflammatory involvement of mesenteric arteries represents a rare but critical etiology.
CTA plays a pivotal role in:
- Identifying arterial wall inflammation and thrombosis
- Assessing bowel viability
- Detecting advanced ischemic changes such as pneumatosis intestinalis and portal venous gas
Recognition of these findings is essential for timely surgical decision-making.
Discussion
AMI most commonly results from embolic or thrombotic occlusion of the SMA. However, large-vessel vasculitis such as Takayasu arteritis can rarely involve mesenteric arteries and their branches.
Inflammatory arterial wall thickening may lead to luminal compromise and predispose to thrombosis. In this case, SMA involvement resulted in thrombosis of multiple distal branches, causing ischemia of corresponding bowel segments.
CT angiography enables simultaneous evaluation of vascular pathology and bowel injury. Imaging features such as absent mural enhancement, pneumatosis intestinalis, and portal venous gas are highly suggestive of severe ischemia and impending or established bowel infarction.
Early recognition of these imaging features is critical for guiding urgent surgical management and improving outcomes.
Conclusion
This case highlights acute mesenteric ischemia secondary to inflammatory thrombosis of superior mesenteric artery branches in Takayasu arteritis.
CT angiography effectively demonstrated arterial wall inflammation, distal branch thrombosis, and advanced ischemic bowel changes including pneumatosis intestinalis and portal venous gas.
Digital subtraction angiography (DSA) plays an important role in the evaluation of mesenteric ischemia by accurately demonstrating the site and extent of vascular occlusion, thereby aiding in the selection of patients for catheter-directed thrombolysis or thrombectomy.
Magnetic resonance imaging (MRI) has a limited role in the assessment of acute mesenteric ischemia because of longer acquisition times and lower sensitivity for bowel ischemia. However, MR angiography (MRA) is valuable for evaluating renal artery patency and renal perfusion, particularly in patients with suspected renovascular disease.
Prompt identification of these characteristic findings is essential for early diagnosis and life-saving intervention.

Dr Ameer Hussain
Consultant Radiologist,
Kauvery Hospital, Chennai.[1]

Dr Manoj C K
1st Year Radiology Resident,
Kauvery Hospital, Chennai.[1]