Abstract:
Hypoxic or ischemic hepatitis is an uncommon consequence of prolonged status epilepticus. We describe a 61-year-old man with a known seizure disorder and poor antiepileptic adherence who presented after an estimated four-hour seizure episode. He developed generalized convulsive status epilepticus, severe lactic acidosis, circulatory shock requiring vasopressin’s, acute kidney injury, rhabdomyolysis, and profound hepatocellular injury. Peak AST and ALT were 9120 U/L and 4327 U/L respectively, with LDH 6056 U/L and INR 4.8. Viral hepatitis testing was negative and imaging showed no structural hepatic abnormality. The clinical and biochemical pattern supported ischemic hepatitis secondary to prolonged seizure activity and systemic hypoperfusion. This case highlights a rare but important complication of status epilepticus.
Introduction:
Status epilepticus is a neurological emergency associated with substantial systemic complications.Prolonged seizures can lead to tissue hypoxia, metabolic acidosis, circulatory instability, rhabdomyolysis, and multiorgan dysfunction. Ischemic hepatitis, also termed hypoxic hepatitis, results from inadequate oxygen delivery to hepatocytes and is most frequently encountered in cardiac failure, septic shock, or respiratory failure. Its occurrence after prolonged convulsive status epilepticus is uncommon and may be under recognized.
Case Presentation:
A 61-year-old male with a known seizure disorder presented to the emergency department following an unwitnessed seizure episode estimated to have lasted approximately four hours. The patient had been prescribed levetiracetam, sodium valproate, and clobazam but was reportedly non-compliant with medications.
At presentation, he was drowsy with a Glasgow Coma Scale (GCS) score of E2V2M6. Subsequently, his neurological status deteriorated to E2V2M1 with ongoing generalized tonic-clonic seizures consistent with convulsive status epilepticus.
Initial Clinical Examination Blood pressure: 90/60 mmHg Heart rate: 150 beats/min
Oxygen saturation: 100% on 4 L/min oxygen GCS: E2V2M1 during active seizures
Given persistent seizures and worsening neurological status, endotracheal intubation and mechanical ventilation were initiated.Routine investigations revealed-
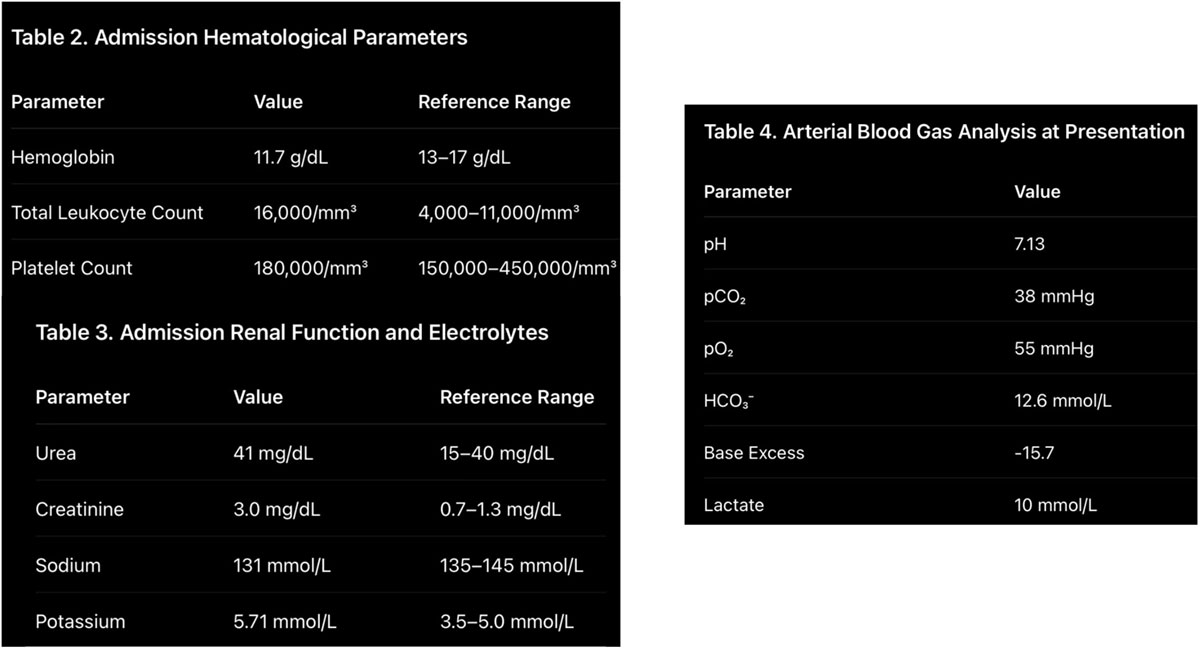
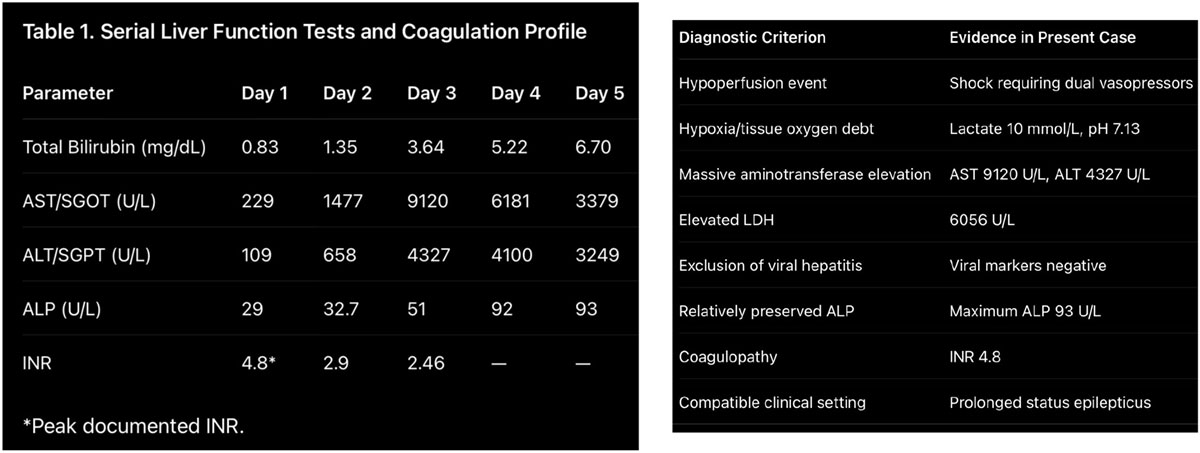
Moreover his initial cranial and abdominal radiology was also unremarkable, Over the ensuing days, he developed marked hepatocellular injury with peak AST of 9120 U/L and ALT of 4327 U/L, associated with progressive hyperbilirubinemia (peak bilirubin 6.7 mg/dL) and severe coagulopathy (peak INR 4.8). Alternative causes of acute liver injury were excluded. The temporal association with prolonged seizures, shock, and profound tissue hypoxia supported the diagnosis of ischemic hepatitis. And also disproportionate rise in transaminases with relatively preserved alkaline phosphatase, together with severe coagulopathy and a compatible clinical setting, strongly suggested ischemic hepatitis.
Management:
The patient was managed in the intensive care unit with: Endotracheal intubation and mechanical ventilation Seizure control using antiepileptic medications Aggressive fluid resuscitation
Vasopressor support for circulatory shock
Correction of metabolic abnormalities with appropriate electrolyte therapy and CRRT
Correction of coagulopathy with appropriate blood products therapy Supportive management for acute liver injury including hepatic encephalopathy measures and acute kidney injury management with CRRT
Discussion:
Ischemic hepatitis is characterized by extensive centrilobular hepatocyte necrosis caused by acute impairment of hepatic oxygen supply. The diagnosis is generally based on three criteria:
*Presence of a clinical condition causing circulatory or respiratory failure.
*Dramatic but transient elevation of aminotransferases.
*Exclusion of alternative causes of acute liver injury. The present patient fulfilled all diagnostic criteria.
Several mechanisms likely contributed to hepatic injury:
*Prolonged seizure activity significantly increase
systemic oxygen demand and metabolic requirements and sustained muscular activity generates profound lactic acidosis and may overwhelm compensatory mechanisms.
*Circulatory Shock- The patient presented with hypotension requiring vasopressor support. Reduced hepatic perfusion particularly affects zone 3 hepatocytes located furthest from the hepatic arterial blood supply.
*Tissue Hypoxia- Despite supplemental oxygen administration, arterial blood gas analysis demonstrated severe hypoxemia (PaO₂ 55 mmHg).
Combined systemic hypoxia and hypotension likely aggravated hepatocellular ischemia.
*Severe Metabolic Acidosis-The lactate level of 10 mmol/L and pH of 7.13 reflected severe tissue hypoperfusion and oxygen debt, both recognized contributors to hypoxic liver injury.
The biochemical pattern was classical for ischemic hepatitis:
-Massive AST elevation (>9000 U/L),
-Marked ALT elevation (>4000 U/L) and
-relatively normal alkaline phosphatase with
-significant coagulopathy
-Progressive but delayed hyperbilirubinemia
An important differential diagnosis was valproate-induced liver injury which was excluded with serum valproate levels which was found to be normal.
And also the abrupt onset following prolonged seizures and shock, the magnitude of transaminase elevation, and the temporal profile were more consistent with ischemic hepatitis than drug-induced hepatotoxicity.
Conclusion:
This case highlights ischemic hepatitis as a rare but potentially severe complication of prolonged generalized convulsive status epilepticus.
The combination of prolonged seizure activity, circulatory shock, profound lactic acidosis, and hypoxemia resulted in massive hepatocellular injury and coagulopathy. Early recognition of ischemic hepatitis in patients with status epilepticus is essential because management is primarily directed at restoring perfusion, correcting hypoxia, and treating the underlying neurological emergency.
Learning Points –
*Status epilepticus can precipitate ischemic hepatitis through systemic hypoperfusion and tissue hypoxia.
*Massive elevations of AST and ALT with relatively normal alkaline phosphatase should raise suspicion for ischemic hepatitis.
*Severe lactic acidosis may serve as an early marker of tissue hypoperfusion and impending organ dysfunction.
*Delayed hyperbilirubinemia does not exclude ischemic hepatitis.
*Prompt seizure control and restoration of hemodynamic stability are critical for preventing secondary organ injury.
*Drug-induced liver injury should be considered but distinguished from ischemic hepatitis based on clinical and biochemical patterns.
*Ischemic hepatitis should be considered when massive transaminase elevation follows prolonged
status epilepticus.
- Elevated LDH and severe coagulopathy strongly support hypoxic liver
- Rhabdomyolysis and acute kidney injury may coexist and indicate severe systemic hypoperfusion.
- Management focuses on correction of the underlying hemodynamic and neurological insult.
References:
- Fuhrmann V, Jäger B, Zubkova A, Drolz Hypoxic hepatitis—epidemiology, pathophysiology and clinical management. Wien Klin Wochenschr. 2010;122(5-6):129-139.
- Henrion J. Hypoxic hepatitis. Liver Int. 2012;32(7):1039-
- Trinka E, Cock H, Hesdorffer D, et A definition and classification of status epilepticus.
Epilepsia. 2015;56(10):1515-1523. - Sutter R, Kaplan Clinical and electroencephalographic correlates of status epilepticus. J Clin
Neurophysiol. 2012;29(5):385-398. - Tapper EB, Sengupta N, Bonder The incidence and outcomes of ischemic hepatitis. Am J
Med. 2015;128(12):1314-1321

Dr Kanagasabai Kamalasekar
Consultant Radiology,
Kauvery Hospital, Chennai.[1]