Abstract
Background: SCAPE is a life-threatening hypertensive emergency.
Case: A 69-year-old male managed with high-dose GTN and NIV.
Conclusion: Early ED intervention prevents intubation.
Introduction
Sympathetic crashing acute pulmonary edema (SCAPE) is a distinct subset of acute heart failure characterized by sudden onset respiratory distress, severe hypertension, and pulmonary edema. The underlying pathophysiology involves acute sympathetic surge leading to marked increase in afterload and redistribution of pulmonary fluid rather than true volume overload.
Conventional management with low-dose vasodilators and diuretics may result in delayed clinical improvement. Recent evidence supports the early use of high-dose intravenous nitroglycerin combined with non-invasive ventilation for rapid hemodynamic stabilization and symptom relief. Studies such as the Hi-Dose SCAPE trial have demonstrated improved outcomes, reduced intubation rates, and shorter emergency department stay with this approach.
This case report highlights the successful application of early aggressive ED-based management using high-dose nitroglycerin and NIV in a patient with SCAPE.
Case Report
A 69-year-old male presented with sudden onset breathlessness of one hour duration (NYHA IV) associated with profuse sweating. He had dull retrosternal chest discomfort for two days.
No history of LOC, Nausea , vomiting , fever, cough, hemoptysis, trauma, syncope, abdominal pain , bowel and bladder disturbances
Primary Survey (ABCDE)
A: Airway patent, drowsy but arousable.
B:B/L AE + , bilateral crepitations , RR : 28 bpm, SpO2 45% on room air.
C:S1 S2 heard , no murmur , PR 140/min, BP 240/130 mmHg., JVP Elevated
D: GCS 14/15, B/L PERL 2 mm , CBG : 377
E: Afebrile, no trauma.
Adjuncts to Primary Survey
| ABG | ON ARRIVAL | After 1 HOUR |
| PH | 6.89 | 7.33 |
| PC02 | 91 | 39 |
| P02 | 72 | 74 |
| Na | 133 | 130 |
| K | 3.7 | 3.8 |
| Cl | 98 | 102 |
| Hco3 | 17.4 | 20.6 |
| Lac | 8.8 | 1.8 |
| Hb | 15.6 | 14.3 |
| Glu | 377 | 325 |
| AG | 21 | 11 |
| BE | -15.7 | -5.3 |
| Fi02 | 61% | 81% |
Creatinine: 1.1 mg/dL.
Troponin I ( Negative ) on Arrival
Repeat Troponin I after 5 Hrs : 1.13 Positive
ECG: Sinus tachycardia
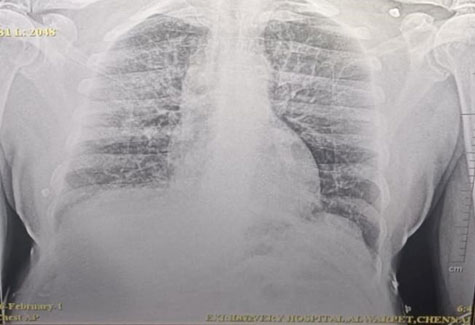
Chest X-ray: Pulmonary Edema
POCUS: B-profile, pleural effusion, dilated IVC, reduced LV function.
Secondary Survey
AMPLE History:
A: No allergies
M: Antihypertensives, OHA
P: DM, HTN
L: Last meal 8 hrs prior
E: Sudden dyspnea
Management
NIV ST – 20:10 ( IPAP:EPAP), FiO2:80%
Inj High-dose NTG at 12 ml/hr with Bolus of 1000 mcg IV stat followed by intermittent bolus were given with strict BP Monitoring
Inj Furosemide 80 mg stat + infusion @ 8 ml/hr
BP monitored every 5 mins.
With Serial BP monitoring ,High dose NTG Dose gradually reduced along with Inj furosemide .
After 3 hrs of Arrival , Patient reassessed , patient symptomatically better .
VITALS: BP 130/80 mmHg / Spo2 : NIV ST 14:7 ( IPAP:EPAP) 100 % Wwith FiO2 : 37%, RR: 24 , PR 86 Bpm Temp : 98.6.
Cardiology consultation obtained and all recommended investigations and therapeutic orders were promptly implemented. After approximately four hours of continuous non-invasive ventilation, the patient was given a trial NIV break under close monitoring. As mild respiratory distress recurred, NIV was restarted, and the patient was subsequently admitted to the coronary care unit (CCU) for further management. Hemodynamic parameters and oxygenation continued to improve over the next 24 hours. On day two of hospitalization, non-invasive ventilation was successfully discontinued, and the patient maintained adequate oxygen saturation on supplemental oxygen.
Discussion
Sympathetic crashing acute pulmonary edema (SCAPE) represents a medical emergency with high risk of respiratory failure and cardiovascular collapse. The predominant mechanism is acute afterload mismatch caused by acute sympathetic activation, leading to rapid pulmonary fluid redistribution, pulmonary congestion, and impaired cardiac output. This pathophysiological process distinguishes SCAPE from subacute volume overload pulmonary edema, which develops gradually over days due to fluid retention and is commonly associated with peripheral edema, weight gain, and relatively stable blood pressure.
Proposed diagnostic criteria for SCAPE include acute onset dyspnea within hours, severe hypertension (systolic blood pressure ≥160 mmHg or mean arterial pressure ≥120 mmHg), respiratory rate ≥30/min, oxygen saturation <90%, and bilateral pulmonary crepitations on examination. These criteria, as described in recent emergency department–based studies, emphasize the importance of early clinical recognition of this distinct phenotype, as management strategies differ substantially from conventional heart failure treatment.
High-dose nitroglycerin exerts both venous and arterial vasodilatory effects, thereby reducing preload and afterload. This results in improved left ventricular performance and rapid resolution of pulmonary edema. The Hi-Dose SCAPE study demonstrated that infusion rates exceeding 100 mcg/min are safe and effective, with a low incidence of hypotension, and are associated with faster symptom resolution and improved clinical outcomes compared with low-dose regimens.
Non-invasive ventilation provides additional benefits by improving oxygenation, reducing preload through positive intrathoracic pressure, and decreasing respiratory muscle fatigue. The combined use of NIV and high-dose nitroglycerin has been shown to significantly reduce intubation rates, ICU admissions, and length of hospital stay. In the present case, early initiation of this combined strategy resulted in rapid clinical improvement and prevention of invasive mechanical ventilation. Continuous monitoring and bedside ultrasonography enabled timely titration of therapy and ensured patient safety.
This case also emphasizes the expanding role of emergency physicians in advanced hemodynamic management, bedside ultrasonography, and protocol-driven care in acute heart failure syndromes, highlighting the importance of early, evidence-based intervention in improving patient outcomes.
Conclusion
Early recognition of SCAPE and aggressive management with high-dose nitroglycerin and NIV in the emergency department leads to rapid symptom resolution and favorable outcomes. Emergency physician-led protocols are crucial in optimizing care in such high-risk presentations.
References
- Houseman BS, Martinelli AN, Oliver WD, et al. High-dose nitroglycerin infusion in SCAPE: safety and efficacy. Am J Emerg Med. 2023;63:74–78.
- Cotter G, Metzkor E, Kaluski E, et al. Randomised trial of high-dose nitrates in pulmonary edema. Lancet. 1998;351:389–393.
- Mathew R, Kumar A, Sahu AK, et al. High-dose nitrates in SCAPE. J Emerg Med. 2021;61:271–277.
- Ponikowski P, Voors AA, Anker SD, et al. ESC Guidelines for Acute and Chronic Heart Failure. Eur Heart J. 2021;42:3599–3726.
- Agrawal N, et al. Sympathetic crashing acute pulmonary edema. Indian J Crit Care Med. 2016.

Dr. Avinash S
Department of Emergency Medicine
Kauvery Hospital, Alwarpet, Chennai.[1]

Dr . Ashok Nandagopal
HOD, Department of Emergency Medicine
Kauvery Hospital, Alwarpet, Chennai.[1]