Abstract
IgA vasculitis, previously known as Henoch–Schönlein purpura, is an immune complex–mediated small vessel vasculitis characterized by deposition of IgA in vessel walls. Although it predominantly affects children, adult-onset disease is relatively uncommon and often presents with atypical manifestations. Gastrointestinal symptoms may precede the characteristic purpuric rash, leading to diagnostic difficulty and potential misdiagnosis.
We report a case of a 62-year-old male who initially presented with symptoms suggestive of acute enterocolitis. Subsequent development of palpable purpura, renal involvement, and histopathological confirmation of leukocytoclastic vasculitis with IgA deposition established the diagnosis of IgA vasculitis. The patient showed significant improvement with systemic corticosteroid therapy. This case highlights the importance of considering vasculitic etiologies in adults presenting with gastrointestinal symptoms associated with purpuric skin lesions.
Introduction
IgA vasculitis (Henoch–Schönlein purpura) is a systemic small vessel vasculitis caused by deposition of IgA-containing immune complexes within vessel walls. The disease typically involves the skin, gastrointestinal tract, joints, and kidneys. It is most frequently encountered in children, with a peak incidence between 4 and 7 years of age. Adult-onset IgA vasculitis is relatively rare but tends to have a more severe clinical course, particularly with regard to renal involvement.
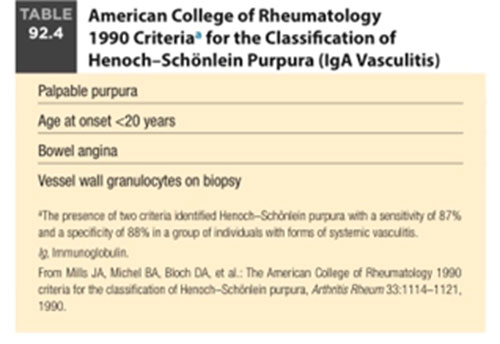
The classical clinical tetrad of IgA vasculitis includes:
- Palpable purpura
- Arthralgia or arthritis
- Abdominal pain
- Renal involvement
Gastrointestinal manifestations are observed in nearly two-thirds of patients and may include abdominal pain, gastrointestinal bleeding, nausea, vomiting, and bowel wall edema. In some patients, gastrointestinal symptoms precede the appearance of the characteristic purpuric rash, which may lead to diagnostic confusion with infectious or inflammatory gastrointestinal disorders.
We present a case of adult-onset IgA vasculitis in which gastrointestinal symptoms dominated the clinical presentation and initially mimicked infective enterocolitis.
Case Presentation
A 62-year-old male with a known history of Type 2 diabetes mellitus and dyslipidemia presented with complaints of loose stools for six days, occasionally mixed with blood, associated with periumbilical abdominal pain, nausea, and intermittent vomiting. The patient also reported bilateral knee pain and generalized fatigue.
On examination, the patient was conscious and oriented. Vital signs revealed tachycardia with a pulse rate of 118/min and hypotension with blood pressure of 80/60 mmHg at presentation. Abdominal examination revealed mild periumbilical tenderness without guarding or rigidity. Cardiovascular and respiratory examinations were otherwise unremarkable.
Dermatological examination revealed multiple non-blanching palpable purpuric lesions over both upper limbs, lower limbs and flanks, predominantly involving the dorsum of the feet and ankles.

Investigations
Hematological Evaluation
- Hemoglobin: 11.4 g/dL
- Total leukocyte count: 9.83 ×10³/µL
- Platelet count: 252 ×10³/µL
Normal platelet counts helped exclude thrombocytopenic causes of purpura.
Renal Function Test was within normal limits and Liver Function Test revealed mild transaminitis
Urinalysis revealed:
- Proteinuria (3+)
- Hematuria (2+), RBCs – 8 to 10 / HPF
Urine protein–creatinine ratio was 1.09, indicating renal involvement.
Immunological Workup
- ANA Profile: Negative
- Anti–double stranded DNA (Anti-dsDNA): Negative
- Anti-Neutrophil Cytoplasmic Antibodies (ANCA):
- MPO-ANCA: Negative
- PR3-ANCA: Negative
- Anti-Glomerular Basement Membrane (Anti-GBM) Antibody: Negative
- Complement Levels:
- C3: Within normal limits
- C4: Within normal limits
- Serum IgA Level: Within normal limits
Stool Examination
Stool examination showed loose stool with mucus. Stool PCR for Clostridium difficile was negative. Stool Occult Blood was Positive
Radiological Findings
Contrast-enhanced CT abdomen demonstrated:
- Long segment small bowel wall thickening involving distal jejunum and proximal ileum
- Surrounding inflammatory fat stranding
- Mild ascites
- No evidence of mesenteric vascular thrombosis
Histopathological Confirmation
Dermatology consultation was obtained and skin biopsy from a purpuric lesion was performed.
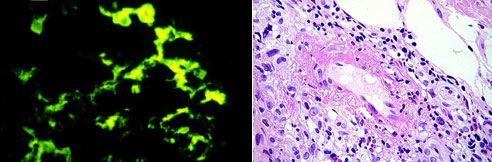
Histopathology revealed orthokeratosis with mild epidermal thinning. Dermal capillaries showed features of small vessel vasculitis, including endothelial swelling and perivascular inflammatory infiltrate predominantly composed of neutrophils and lymphocytes with extravasation of red blood cells.
Direct immunofluorescence showed granular IgA (2+) and C3 (1–2+) deposition in superficial dermal capillaries, confirming the diagnosis of IgA vasculitis.
Treatment
The patient was treated with systemic corticosteroid therapy.
In-hospital treatment
- Inj. Dexamethasone
- Proton pump inhibitors
- Probiotics
- Supportive care
Following clinical improvement, the patient was discharged on:
- Tab. Prednisolone 30 mg once daily followed by tapering dose
Outcome and Follow-Up
At follow-up evaluation:
- Cutaneous lesions showed significant resolution
- Gastrointestinal symptoms resolved completely
- Renal function tests remained normal
- No new purpuric lesions were noted
The patient demonstrated a good clinical response to corticosteroid therapy.
Discussion
IgA vasculitis is an immune complex–mediated small vessel vasculitis characterized by deposition of IgA within vessel walls. While the disease predominantly affects children, adult cases are increasingly recognized and often demonstrate more severe systemic involvement.
Gastrointestinal involvement occurs in approximately 50–85% of cases and may present as abdominal pain, gastrointestinal bleeding, nausea, vomiting, or bowel wall edema. Radiological findings typically include segmental small bowel thickening and mesenteric edema, which may mimic infectious or inflammatory gastrointestinal conditions.
In the present case, gastrointestinal manifestations preceded the recognition of systemic vasculitis, leading initially to a diagnosis of infective enterocolitis. The subsequent development of palpable purpura and renal abnormalities prompted evaluation for vasculitis. Skin biopsy with demonstration of IgA deposition remains the gold standard diagnostic test.
Early recognition and initiation of corticosteroid therapy can lead to rapid symptomatic improvement and may reduce the risk of complications such as gastrointestinal bleeding or renal impairment.
Learning Points
- Adult-onset IgA vasculitis is uncommon and may present atypically.
- Gastrointestinal manifestations may precede cutaneous findings.
- Palpable purpura with normal platelet counts should prompt evaluation for small vessel vasculitis.
- Skin biopsy with IgA deposition confirms the diagnosis.
- Corticosteroid therapy can lead to rapid symptom resolution.
References
- Pillebout E, et al. Henoch–Schönlein Purpura in adults: outcome and prognostic factors. Journal of the American Society of Nephrology.
- Jennette JC, Falk RJ. Small-vessel vasculitis. New England Journal of Medicine.
- Audemard-Verger A, et al. IgA vasculitis in adults: clinical features and management. Autoimmunity Reviews.
- Watts RA, et al. Nomenclature and classification of vasculitis. Annals of the Rheumatic Diseases.

Dr. S. Akash Kumar
DNB Resident, General Medicine
Kauvery Hospital, Chennai.[1]

Dr. S. Sivaram Kannan, MBBS., MD(Gen Med)., FRCP(Glasgow)
Clinical Lead & Chief Consultant Physician, General Medicine
Kauvery Hospital, Chennai.[1]

Dr. S. Sham MBBS., MD(Gen Med)., DM(Rheumatology)., MRCP(UK)., FRCP(Edin)., SCE (RCP UK) European Certificate of Rheumatology
Senior Consultant, Rheumatology
Kauvery Hospital, Chennai.[1]

Dr. Vijay Kartik MBBS., D.V.D
Consultant, Dermatology
Kauvery Hospital, Chennai.[1]