Abstract
Tracheal stenosis is a rare but potentially life-threatening condition that may develop following prolonged or traumatic endotracheal intubation. We present a case of a 34-year-old male who developed progressive respiratory distress due to subglottic stenosis one month after an episode of status epilepticus requiring intubation. This case highlights the importance of early recognition, appropriate post-intubation care, and timely intervention in preventing and managing airway stenosis.
Case Report
A 34-year-old male presented to the Emergency Department with complaints of progressive shortness of breath (NYHA Class II–III) for the past three days, worsened on exertion, and associated with a dry cough. He had been evaluated at an outside clinic two days earlier and was treated symptomatically for a lower respiratory tract infection with nebulization, without significant relief.
No H/o LOC/Giddiness/ Chest pain / palpitation/Fever/chills & rigor / nausea / vomiting /abdominal pain / bowel & bladder disturbances
Past Medical History
The patient was a known case of seizure disorder, with a recent hospital admission one month prior (11/08/2025) for status epilepticus. He was intubated at an outside hospital and subsequently transferred to our Emergency Department for further management. He was extubated on day 2 of admission, antiepileptic medications were titrated, and he was discharged on 16/08/2025.
Type II Diabetes mellitus
Examination
On arrival, Concious/oriented/afebrile
Airway (A): Patent, audible wheeze present/ Stridor +
Breathing (B): Bilateral air entry present, B/L Diffuse wheeze ++
Circulation (C): S1, S2 present, no murmurs.
Disability (D): GCS 15/15, moving all four limbs.
Exposure (E): Temperature 98.6°F.
Throat: No congestion, no tongue swelling, no angioedema
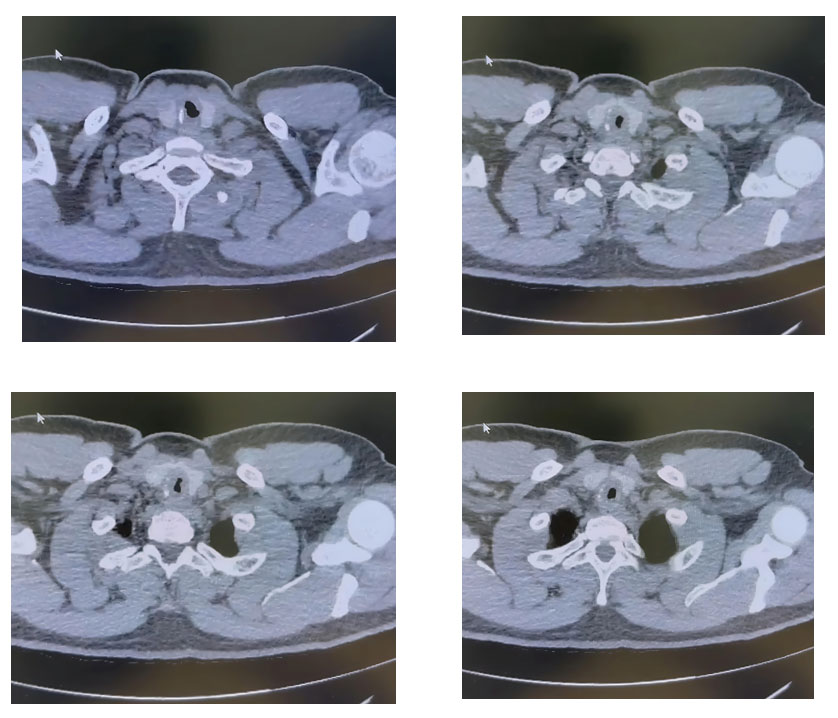
Investigations
A CT Neck and Chest revealed a severe short-segment tracheal narrowing at the C7 level, suggestive of subglottic stenosis.
Diagnosis
Post-intubation subglottic stenosis (PISS).
Discussion
Anatomy and Classification
The trachea extends from the subglottic region of the larynx to the carina, bifurcating into the main bronchi.
Subglottis: Region just above the trachea, below the vocal cords, lacking cartilage rings.
Glottis: Contains the vocal cords. Supraglottis: Region above the glottis extending to the base of the tongue.

Stenosis can be categorized as:
- Laryngeal/Laryngotracheal stenosis
- Tracheal stenosis
- Tracheobronchial/Bronchial stenosis
Clinical Features
Symptoms vary with severity and may include dyspnea, wheeze or stridor, cough, hemoptysis, dysphonia, or dysphagia. Symptoms usually develop 3–6 weeks post-extubation in post-intubation tracheal stenosis (PITS).
Etiology
- Internal (Post-Intubation / Post-Tracheostomy): Pressure necrosis from the endotracheal or tracheostomy tube cuff, traumatic or prolonged intubation.
- External: Blunt or penetrating neck trauma, inhalational or chemical injury, foreign body aspiration.
- Inflammatory/Systemic Causes: Vasculitis (GPA, MPA, RA), SLE, Inflammatory bowel disease.
- Infectious Causes: Mycobacterial (Tuberculosis), Fungal (Aspergillus, Histoplasma), Viral (HSV, CMV, HPV), Bacterial (Staphylococcus aureus, Mycoplasma pneumoniae, Corynebacterium, Haemophilus influenzae).
- Others: Nonmalignant tumors, congenital or idiopathic causes, radiation-induced fibrosis, extrinsic compression.
Management
Acute management includes nebulized adrenaline and corticosteroid’s to reduce inflammation and edema.
Definitive management:
- Endoscopic interventions: Balloon dilation, laser ablation, or stent placement.
- Surgical options: Tracheal resection and reconstruction for refractory cases.
- Tracheostomy: For severe or recurrent stenosis.
In the present case, pulmonology and ENT consultations were obtained, and the patient was treated with nebulized adrenaline. IV hydrocortisone (100 mg), and IV dexamethasone (8 mg) were advised. Emergency tracheostomy and bronchoscopy-guided dilatation were planned; however, the patient and family declined further intervention and discharged against medical advice (DAMA).
Post-Intubation Care and Prevention of Tracheal Stenosis
Proper post-intubation care is vital in preventing airway injury and subsequent stenosis:
- Appropriate tube size selection to minimize mucosal trauma.
- Monitoring cuff pressure (should not exceed 25–30 cm H₂O) to prevent ischemic injury.
- Avoidance of unnecessary movement of the endotracheal tube.
- Regular suctioning and humidification to prevent secretion buildup.
- Early extubation whenever feasible.
- Surveillance bronchoscopy in patients with difficult or prolonged intubation.
- Timely recognition of post-extubation symptoms like exertional dyspnea, stridor, or unexplained wheeze, which warrant airway evaluation.
Conclusion
Post-intubation subglottic stenosis is a potentially serious but preventable complication. Early recognition of airway symptoms following extubation and meticulous post-intubation care are essential to prevent morbidity. Collaborative management involving emergency physicians, pulmonologists, and otolaryngologists ensures the best outcomes.
References
- Grillo HC. Development of tracheal surgery: A historical review. Ann Thorac Surg. 2003;75(2):610–619.
- Whited RE. Posterior commissure stenosis post long-term intubation. Laryngoscope. 1983;93(10):1314–1318.
- Zias N, et al. Postintubation tracheal stenosis: Risk factors and prevention. Chest. 2008;134(3):539–546.
- D’Andrilli A, et al. Post-intubation tracheal stenosis: Surgical treatment and long-term results. Eur J Cardiothorac Surg. 2016;50(3):411–417.
- Nouraei SA, et al. Impact of perioperative care on outcomes in post-intubation laryngotracheal stenosis. Laryngoscope. 2007;117(8):1425–1431.

Dr. Avinash S
Department of Emergency Medicine,
Kauvery Hospital, Alwarpet, Chennai.[1]

Dr . Ashok Nandagopal
HOD , Department of Emergency Medicine,
Kauvery Hospital, Alwarpet, Chennai.[1]