Introduction

Acute limb ischemia (ALI) is one of the medical emergencies where time literally is money. Prompt diagnosis and intervention within the golden hours (6-8) before the tissues become irreversibly damaged ensure the best outcome for the patient.
In most cases, the symptoms of ALI are severe and the signs characteristic. However, failure to do a proper clinical examination or elicit relevant history may cause missed diagnoses of ALI.
Case Profile and Clinical Progression
We present a case where a 45-year-old female initially had severe pain in her left lower leg and feet with some degree of weakness. She promptly sought treatment and was administered pain killers and advised to get MRI of spine. Her pain continued to worsen and by day 5 she had started to develop skin changes with restriction of toe movements. Unfortunately, a proper pulse examination wasn’t done, and she went on to develop calf tenderness and skin mottling – telltale signs of irreversible ischemia.

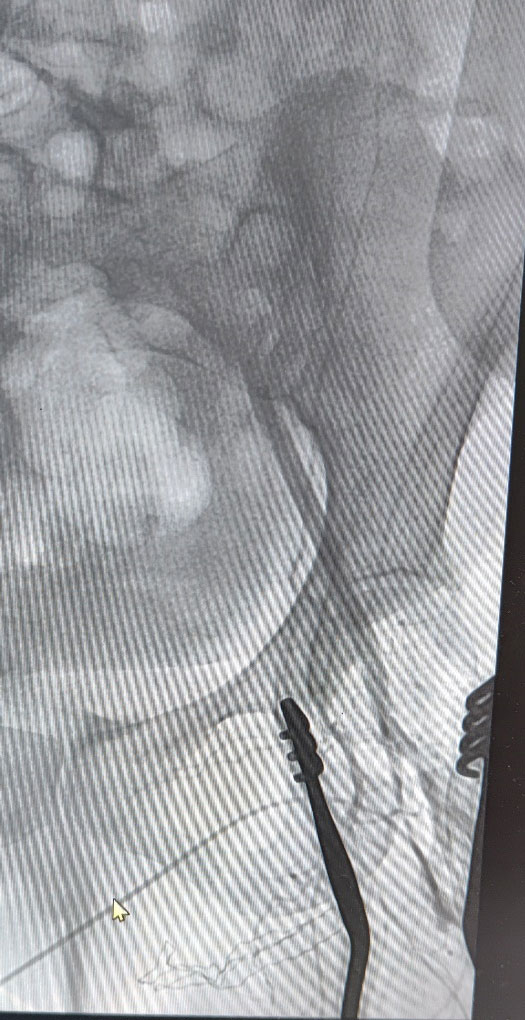
When she came to the Vascular Surgery Department, her left leg had color changes of the skin up to the lower 3rd of the leg, hypothermia till mid leg, flickers of movement at the ankle and absent left lower limb pulses. CT angiogram of the lower limb demonstrated thrombus in the iliac artery, occluded common and superficial femoral arteries and scant reformation of the tibial arteries. The prognosis was explained to the patient and attenders and emergency femoral and if needed, popliteal thrombectomy was offered as a last-ditch effort to save the leg. As the presentation was very much delayed, high probability of failure and need for major amputation were stressed upon.
The image shows the CT angiogram of the patient showing occluded iliac and femoral arteries. The tibial arteries are poorly visualized as well. Note the relatively well-preserved right-side vasculature.

Surgical Procedure
She underwent emergency left transfemoral thrombectomy and puncture angiogram of the left iliac artery at the hybrid cath suite. Chronic thrombus was retrieved from the iliac and femoral artery and evidence of a proximal (iliac) occlusion was seen in the angiogram. It was akin to keeping a sinking ship afloat as she kept thrombosing again and again on table even after multiple thrombectomies. Further attempts were stopped, and she was maintained on high dose IV anticoagulation while investigations were done to deduce a cause for thrombophilia. She was found to have thrombocytosis. Her cardiac system was normal and there was no source of emboli upstream. The left leg developed progressive gangrene, and she had to undergo a below knee amputation of her left leg.

Managing Acute Limb Ischemia
ALI usually presents dramatically with a sudden onset of severe pain that is sometimes associated with weakness. Patients often remember the exact time of occurrence and can often recollect the activity they were engaged in at the time of onset. An embolus at the bifurcation of aorta can cause paraplegia that can easily be mistaken for a stroke. Examination should be comprehensive assessing all peripheral pulses and the contralateral extremity should always be compared with. In advanced ischemia, tissues will appear cyanotic, clammy with reduced sensations and movements will be restricted. Foot drop, skin mottling and calf turgor with tenderness indicate ischemia with likely irreversible damage. Those with delayed presentation are also at risk of acute kidney injury, acute coronary events and multi-organ failure. Rutherford’s classification of ischemia helps in deciding on the type of management.
Imaging – duplex USG, CT angiogram or MR angiogram help in operative planning. Basic blood investigations – hemogram, renal functions, serum homocysteine and coagulation profile are done. A transthoracic echocardiogram is done to rule out cardiac emboli.
Traditionally, thrombectomy/embolectomy was done to revascularize. Bypasses with reversed saphenous vein or a prosthetic graft are sometimes required when the thrombus is chronic and thrombectomy fails. ALI is also managed with endovascular interventions which include catheter directed thrombolysis, thrombosuction, angioplasty and stenting. Patients with ALI tend to have other comorbidities as well – diabetes, hypertension, dyslipidemia, thrombophilia, CAD, CVD and addictions. Involving other specialties will give better outcomes.
Avoiding Such Costly Mistakes
An act as simple as touching her feet to feel for pulses could have possibly changed the entire episode and avoided the amputation. The patient’s complaints and observations always warrant proper attention and scrutiny. When the treatment administered doesn’t evoke expected outcomes, it’s better to pause and strategize better. The patient and the attenders should always be informed about progress or deterioration and given realistic expectations about the outcomes. After all, acute limb ischemia is unforgiving and takes no prisoners.

Dr. Jan Sujith
Associate Consultant Vascular Surgery,
Kauvery Hospital, Chennai
கடவுளின் அருளும், டாக்டரின் கைவினையும்
என் பெயர் ஹேமாவதி. என்னுடைய வயது 79. எனக்கு 2013ல் L4, L5 அழுத்தத்தினால் இடுப்பு வலியோடு இடது கால் மறுத்துப் போனது. அதன் பின் ஆபரேஷன் செய்யாமல் மூன்று மாத ஓய்வுக்குப் பின் சிறிது குணமானது. அதன்பின் கால் கருப்பு நிறமாகவும், அரிப்பும் ஏற்பட்டு சிகிச்சை எடுத்து பலனில்லாமல் வெரிகோஸ் டாக்டரைப் பார்த்து, அவர் பரிந்துரைப்படி சாக்ஸ் போட்டு, மாத்திரைகள் சாப்பிட்டு, கிரீம்கள் போட்டும் வீக்கம், நரம்பு சுருட்டல் சரியாகாமல் டாக்டர் சேகர் அவர்களிடம் சிகிச்சை எடுத்து, நேற்று லேசர் சிகிச்சை செய்து கொண்டேன். கடவுள் அருளும் டாக்டர் சிகிச்சையும் நல்ல பலன் அளிக்கும் என நம்புகிறேன்.
We had great experience and best treatment by Dr.N.Sekar, Chief Vascular Surgeon at Kauvery Hospital, Alwarpet, Chennai.
My wife Mrs.Thenral Manoharan after Doppler scan, CT scan diagnosed with poor blood circulation (Ischemia) in her right lower limb. Due to this she had heel pad ulcer wound with heavy pain.
Dr. Sekar performed CDT, bypass surgery and explanation of Graft.
Dr.Sekar’s commitment to patient care and innovative approach to treatment was great. He is expertise in vascular treatment and enabled my wife to get ulcer wound cure and walk normally without amputation. He saved her leg and life. After his treatment, the blood flow found normal.
He is one of the most meticulous surgeons in the field of Vascular surgeries. Dr.N.Sekar dedication to excellence and his passion for improving patient outcomes have made him most trusted and respected Vascular Surgeon in Tamil Nadu.
This is Mohammed Mubeen from Vedasandur, Dindigul district, Tamil Nadu . My father (Rizwan Ahamed) leg infection and was Diabetes for few months and for that we have been to Dr. Sekar
Vascular surgeon (Kaveri hospital) for treatment , he has recovered almost now.
It’s a great honour even to write about you, most importantly the way you try to improve yourself as a better doctor on a day-to-day basis and keeping in touch with your patients is so heart touching.
I strongly believe doctor is not someone who just cure illness of the patient but also boosts the morale of the patient so that they can feel much better than ever. it was there in your treatment for sure. What else can one ask for from a doctor.
To put simple about how to express my gratitude – No one wants to see a doctor being a patient, but it’s worth to keep in contact with someone like you who is a well-established overall person.
It’s so good to see my father come back to normal, thanks for your treatment with personal care.
Thanks for your support, sir. May God bless you.
