
Introduction
Chronic liver disease (CLD) progresses through fibrosis → cirrhosis, irrespective of etiology (viral, alcohol, NAFLD, autoimmune). Accurate staging of fibrosis is essential for:
- Prognosis
- Treatment planning
- Monitoring disease progression
Traditionally, liver biopsy is the gold standard, but it is invasive and limited by sampling error. Hence, elastography has emerged as a non-invasive, reliable alternative.
Need for Elastography
Limitations of Liver Biopsy
- Invasive, risk of haemorrhage
- Sampling error (heterogeneous fibrosis)
- Interobserver variability
- Not suitable for follow-up
Limitations of Conventional Imaging
- CT/MRI/US detect late cirrhosis only
- Poor sensitivity for early fibrosis
Hence, elastography bridges the gap by quantifying tissue stiffness.
Basic Principle of Elastography
Elastography measures tissue stiffness based on:
- Stress → applied force
- Strain → tissue deformation
Fibrotic liver = stiffer tissue → faster wave propagation
Types of Liver Elastography
Ultrasound-Based Elastography:
-
Strain Elastography
- Uses manual compression
- Qualitative (colour map)
- Limited role in the liver
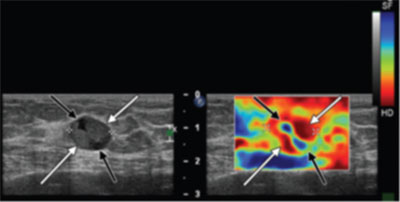
Strain elastography shows a complex cystic-solid lesion with mixed stiffness – the solid component appears stiff (red) and cystic component appears soft (blue).
-
Transient Elastography (FibroScan)
- Uses mechanical vibrator (50 Hz)
- Measures stiffness in kPa
- No real-time imaging
Advantages:
- Fast (<5 min)
- Bedside technique
Limitations:
- Not usable in ascites
- Limited in obesity
- No B-mode guidance
-
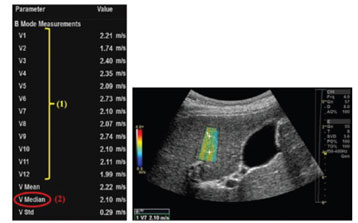
Point Shear Wave Elastography (pSWE)
- Uses acoustic radiation force impulse (ARFI)
- Measures velocity (m/s)
- ROI-based
-
2D Shear Wave Elastography
- Real-time colour elastogram
- Larger ROI
- Better spatial mapping
MR Elastography (MRE)
- Uses mechanical waves (60 Hz)
- Measures shear modulus (kPa)
- Produces:
- Wave images
- Elastogram (stiffness map)
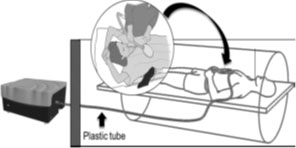
MR elastography setup showing an external acoustic wave generator transmitting vibrations via tubing to a passive driver placed on the patient’s abdomen.

Technique
US Elastography
- Supine/left posterior oblique position
- Right lobe via intercostal approach
- Breath-hold (end expiration)
- 10–12 measurements; median value used
MR Elastography
- Passive driver over the right lobe
- 4 axial slices acquired
- ROI avoids capsule, vessels, artifacts
Interpretation
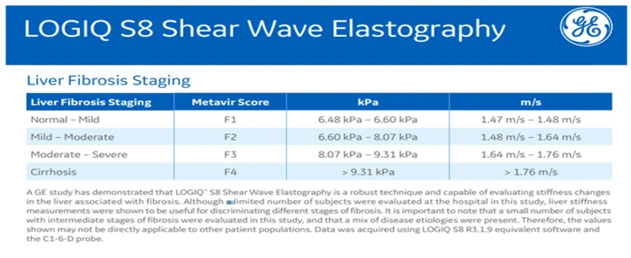
US Elastography
- Low → F0–F1
- Intermediate → F2–F3
- High → F4 (cirrhosis)
- Machine-dependent cutoffs
MR Elastography (kPa)
- <2.5: Normal
- 2.5–2.9: Inflammation
- 2.9–3.5: F1–F2
- 3.5–4.0: F2–F3
- 4–5: F3–F4
- 5: Cirrhosis
Confounding Factors
Technical
- Incorrect ROI
- Left lobe (false high)
- Depth > 7 cm (false low)
- Inclusion of vessels/capsule
Biological
- Inflammation
- Congestion
- Postprandial state
- Alcohol
Clinical Applications
- Fibrosis staging
- Treatment monitoring
- Portal hypertension prediction
- NAFLD/NASH evaluation
- Transplant assessment
Advantages & Limitations
Advantages
- Non-invasive, repeatable
- Large sampling volume
- Early fibrosis detection
Limitations
- Operator-dependent (US)
- Lack of standardization
- Cost (MRE)
- Cannot determine etiology
Future Directions
- Spleen stiffness for portal HTN
- Tumour characterization
- Fibrosis vs inflammation differentiation
- Prognostic biomarker
Conclusion
Elastography is a non-invasive, accurate, and reproducible tool for liver fibrosis assessment, reducing reliance on biopsy.

Dr Kanagasabai Kamalasekar
Consultant Radiology,
Kauvery Hospital, Chennai

Dr Malavika S
DNB Radiology Resident,
Kauvery Hospital, Chennai
