
Venous thromboembolism is the third most common cardiovascular disease and primarily manifests in two forms, i.e. deep vein thrombosis (DVT) and pulmonary embolism (PE) [1,2].
People who are more prone to DVT are as follows:
- Age more than 50 years
- BMI > 35
- Postpartum period
- History of prior venous thromboembolism
- Recent surgery
- Immobility
- Major trauma
- Smoking
- Stroke
- Cancer
- Leukaemia
- Thrombophilia
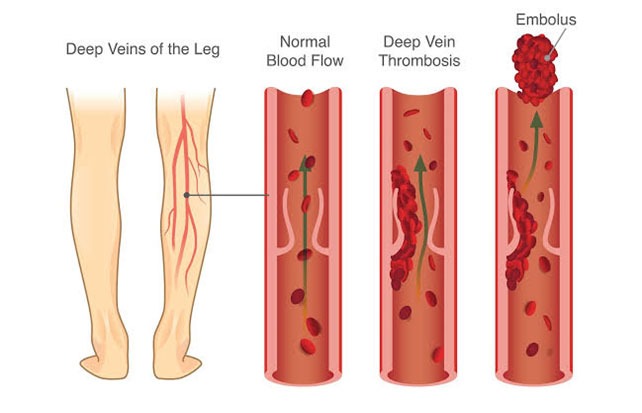
Image 1: Shows how a DVT is formed and how it can dislodge an embolus to cause a more potentially fatal PE.

Image 2: Shows the difference between a normal leg and a leg with deep vein thrombosis marked with an arrow. We can appreciate the affected leg to be more swollen and redder compared to the normal leg.
Accurate lower extremity DVT diagnosis and treatment is crucial because it carries a risk of developing into a potentially fatal pulmonary embolism. Deep vein thrombosis commonly originates in the leg veins. Traditional clinical signs such as Homan’s sign, edema and tenderness are not reliable indicators of DVT because of their non-specific nature [3,4]. Laboratory tests like D-dimer aid in diagnosing but it is non-specific in nature. Then came CT venography which once was considered a gold standard for diagnosis but it is invasive and painful with risks of radiation exposure and insufficient contrast enhancement. Traditional whole-leg ultrasound is non-invasive and is the primary diagnostic method for deep vein thrombosis, but the limitation here is that it is not available 24/7, compelling patients to stay in the emergency department until standard working hours.
The recently performed lower limb venous point-of-care ultrasound (POCUS) by emergency physicians has improved the time to diagnose deep vein thrombosis.
The protocol for 3-point lower extremity venous POCUS involves the following vascular landmarks, namely:
S1 – From superior to common femoral vein to great saphenous vein bifurcation
S2 – Proximal superficial and deep femoral vein segment
S3 – Popliteal vein to the trifurcation
Also, if there is a suspicion of DVT, the vein is gently compressed with the ultrasound probe. The “Uncompressible” nature of the vein confirms DVT.
Image 3: Shows an ultrasound machine used to do point-of-care ultrasound in the Emergency Department.

Image “A” – Black zones show the scanning areas to identify DVT.
Image “B” – Shows the common femoral artery and common femoral veins. The common femoral vein displays a thrombus in its lumen making it uncompressible.

This ultrasound is focussed on two or three specific sites and has demonstrated an accuracy compatible with that of specialists and is significantly faster [5,6,7,8]. Despite these advantages, there is a research gap in defining the ultrasound experience level required by the emergency physician to achieve specialist-level accuracy. But detection when under suspicion of DVT always improves the time to initiation of prompt treatment leading to less morbid and more favourable outcomes. We at Kauvery Hospitals have consultant emergency physicians equipped with these skills. If there is a suspicion of DVT in patients, POCUS is done immediately by emergency physicians in the emergency department to promptly diagnose DVT and initiate treatment at the earliest.
References:
1 – Goldhaber SZ, Bounameaux H. Pulmonary embolism and deep vein thrombosis. Lancet. 2012;379:1835–46.
2 – Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ. 3rd. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998;158:585–93.
3 – Kearon C, Julian JA, Newman TE, Ginsberg JS. Noninvasive diagnosis of deep venous thrombosis. McMaster Diagnostic Imaging Practice Guidelines Initiative. Ann Intern Med. 1998;128:663–77.
4 – McLachlin J, Richards T, Paterson JC. An evaluation of clinical signs in the diagnosis of venous thrombosis. Arch Surg. 1962;85:738–44.
5 – Pomero F, Dentali F, Borretta V, et al. Accuracy of emergency physician-performed ultrasonography in the diagnosis of deep-vein thrombosis: a systematic review and meta-analysis. Thromb Haemost. 2013;109:137–45.
6 – Farahmand S, Farnia M, Shahriaran S, Khashayar P. The accuracy of limited B-mode compression technique in diagnosing deep venous thrombosis in lower extremities. Am J Emerg Med. 2011;29:687–90.
7 – Pedraza Garcia J, Valle Alonso J, Ceballos Garcia P, Rico Rodriguez F, Aguayo Lopez MA, Munoz-Villanueva MDC. Comparison of the Accuracy of Emergency Department-Performed Point-of-care-ultrasound (POCUS) in the diagnosis of lower-extremity deep vein thrombosis. J Emerg Med. 2018;54:656–64.
8 – Elsenga HE, Collee A, Rosendaal AV. Agreement between emergency physicians and radiologists for the diagnosis of deep venous thrombosis with compression ultrasound: a prospective study. Eur J Emerg Med. 2021;28:25–8

Dr. Karunakaran Vetri
Consultant Emergency Physician,
Department of Emergency Medicine,
Kauvery Hospital, Chennai
