Diabetes Mellitus and the Kidney
Introduction:
Diabetic nephropathy is a kidney disease that results from diabetes. It is the number one cause of kidney failure. Almost a third of people with diabetes develop diabetic nephropathy. People with diabetes and kidney disease do worse overall than people with kidney disease alone. People with diabetes are also more likely to have other kidney-related problems, such as urinary tract infections and neuropathic bladder. It is the leading cause of chronic kidney disease in India as well as in the rest of the world.

Diabetic nephropathy develops in 40% of patients with Type 2 diabetes mellitus and 30% of patients with Type 1 diabetes. The prevalence is continuously rising with disparate growth in low to middle-income countries and under-recognized as a global disease burden. It is also associated with a high mortality rate. Additionally, it imposes an enormous humanistic, economic and societal burden. The major hurdle in the early diagnosis is limited knowledge and urine routine screening.
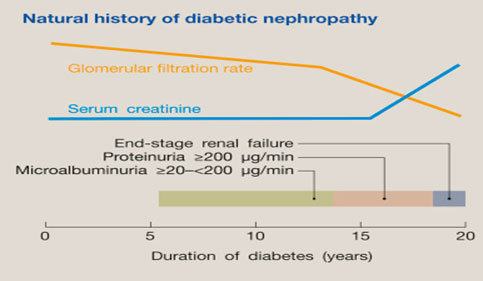
Natural History
Kidney disease in Type 1 diabetes is slightly different than in Type 2 diabetes. In Type 1 diabetes, kidney disease rarely begins in the first 10 years after diagnosis of diabetes. The classical Mogensen classification of stages of diabetic nephropathy belongs to Type 1 diabetes mellitus.
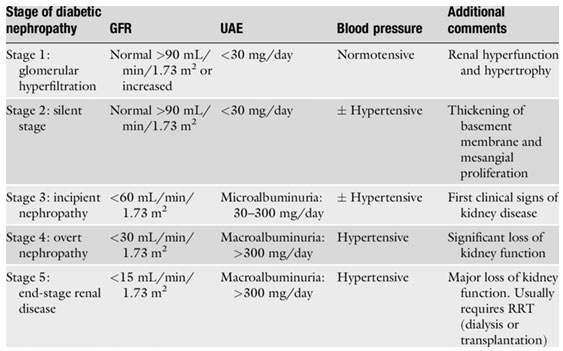
Table 1: Stages of Diabetic Nephropathy in Type 1 Diabetes Mellitus
In Type 2 diabetes mellitus, the natural disease is most often altered due to associated high blood pressure, dyslipidemia, ischemic heart disease/cardiac disease and recurrent urosepsis.
The onset of Type 1 diabetes mellitus is more defined from a set period from childhood days and hence one can predict the onset of diabetic nephropathy in a Type 1 diabetic which is 5 to 10 years from the time of diagnosis. Type 2 diabetes mellitus is most often undetected and many patients are diagnosed with diabetic nephropathy at the time or within a short time of diagnosis, as they would have had undetected hyperglycemia before.
The natural history is characterized by no symptoms till stage 3 and later stages 4 and 5 have symptoms of hypertension and edema due to proteinuria.
Symptoms and Signs of Diabetic Nephropathy
- Usually asymptomatic in the early stages
- Edema – Swelling of the legs due to macroalbuminuria
- Breathlessness due to pulmonary edema
- Decreased urine output
- Hypertension
- Blurring of Vision – Due to diabetic retinopathy
Nearly 90% percent of diabetic nephropathy patients have associated diabetic retinopathy. In fact, the absence of diabetic retinopathy in a patient with nephropathy in a diabetic should alert the alarm for non-diabetic glomerular diseases.
Investigations:
Annual urine routine examination with urea, creatinine and serum electrolytes is recommended for all diabetic patients as early diabetic nephropathy involvement is missed in the asymptomatic stages.
24-hour urine estimation which was the gold standard in the quantification of proteinuria, has been replaced by the less cumbersome urine spot protein creatinine ratio. USG whole abdomen usually shows normal-sized kidneys in diabetic kidney disease.
Treatment
The goal of treatment is to prevent the progression from micro- to macroalbuminuria, the decline of renal function in patients with macroalbuminuria, and the occurrence of cardiovascular events.
- Intensive blood glucose control to achieve HbA1c of 6.5%.
- Normalizing of blood pressure to 130/85 mm of Hg in microalbuminuria patients and 120/80 mm in patients with macroalbuminuria – RAAS blockade is the mainstay of the therapy.
- Dyslipidemia management to achieve the targets as in high-risk cardiovascular disease (LDL‹100 mg%).
- Normal levels of uric acid by uricosuric agents like febuxostat or allopurinol.
- Salt and water restriction in the diet and to treat with diuretics if volume overloaded.
- Maintain normal levels of serum bicarbonate (23-26 mEq/L).
- Protein restriction in the diet by restricting animal protein.
- SGLT2 inhibitors (sodium glucose cotransporter inhibitor) – Dapagliflozin, canagliflozin, empagliflozin – reduce the hyperfiltration injury, reduce glucose levels, reduce blood pressure by causing natriuresis.

Dr R Balasubramaniyam,
Chief Nephrologist
Department of Nephrology,
Kauvery Hospital, Chennai

Dr Balaji Kirushnan,
Consultant Nephrologist
Department of Nephrology,
Kauvery Hospital, Chennai
