Introduction

Primary hyperparathyroidism (PHPT) is an endocrine disorder characterized by elevated or normal serum calcium levels in the presence of elevated or inappropriately normal parathyroid hormone (PTH) levels. The incidence varies from 0.4 to 82 cases per 100,000. Females account for about three-fourths of all cases but the incidence rates are similar in men and women less than 45 years of age.
What Causes Primary Hyperparathyroidism?
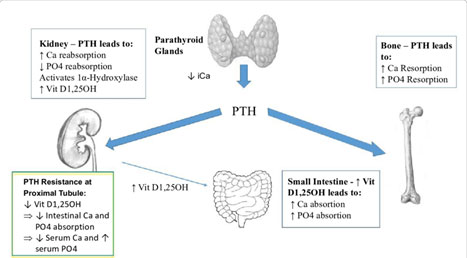
Regulation of Calcium Homeostasis
Clinical Phenotypes of PHPT:
The clinical and biochemical profile of PHPT varies in different parts of the world.
- Symptomatic PHPT – Associated with overt skeletal and renal complications. In India, > 90% of the patients present with symptomatic disease compared to the West, where asymptomatic disease has been the dominant clinical phenotype.It has a varied clinical presentation which includes:
- Asymptomatic PHPT – No overt symptoms or signs, typically discovered by biochemical screening. On evaluation, target organ involvement may or may not be present.
- Normocalcemic PHPT – Precursor or subclinical form of classical PHPT.
PHPT – Indian Scenario
- Primary hyperparathyroidism (PHPT) in the Indian population has a wide spectrum of clinical presentations.
- Most common presentations include generalized weakness (80%), bone pain (35%) and renal stone disease (20%).
- Asymptomatic disease is seen in 15% of the patients.
Who’s Most at Risk?
Diagnosing Primary Hyperparathyroidism
| Forms of Hyperparathyroidism | Serum Calcium | PTH Level | Phosphate Level | 24 Hour Urinary Calcium Level |
| Primary HPT | Increased | Raised | Low | Ø 300-400 mg/day |
| Secondary HPT | Normal/Low | Raised | Low – Vitamin D deficiency
High – Renal failure |
Depends on cause |
| Tertiary HPT | Increased | Raised | Variable | Low before transplant |
| Normocalcemic PHPT | Normal | Raised | Normal | < 350 mg/24 hours |
| Familial Hypocalciuric Hypercalcemia (FHH) | Increased | Raised | Normal | < 100 mg/day |
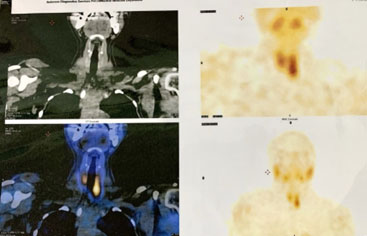
Pre-Operative Localisation
Treatment

- Most PHPT features are likely to improve with a surgical cure.
- Surgery is the only curative treatment, is cost-effective and is indicated for all symptomatic patients.
- Surgical options include:

Dr. Dhalapathy Sadacharan
Consultant Surgical Endocrinologist,
Kauvery Hospital, Chennai
