A timely biopsy saves life
Abstract
Background: We present a case of non healing ulcer of foot in an elderly male patient who was a known diabetic. The ulcer was treated for more than 3 months outside as diabetic ulcer in outside hospital. Patient had visited our plastic surgery OPD, was subjected to biopsy and was diagnosed as Malignant melanoma. Then patient was subjected to further evaluation and referred to oncology team. This journal discusses the importance of timely biopsy that has a huge impact on this most aggressive skin cancer.
Key words: Melanoma; Diabetes mellitus; Edge wedge biopsy
Introduction
The incidence of primary cutaneous melanoma has increased steadily for several decades and is one of the lethal form of cutaneous neoplasm. If diagnosed in the early stages, melanoma has high survival rates, approximating 94%.[1] Melanoma was once considered a very aggressive cancer that was resistant to traditional therapies such as chemotherapy, radiation, and even single-agent targeted therapies in their early stages of development. A dramatic improvement in the quality of life and overall survival of patients with metastatic melanoma has resulted after the advent of various new combinations of targeted therapies and different modalities of immunotherapies. [2]
Case Presentation
A 52-year-old male patient was treated in outside hospital for an ulcer in left foot. Patient was a known case on diabetes mellitus and was getting treated for the same. The ulcer wound was diagnosed as diabetic foot ulcer. Patient had been receiving regular dressing and was on diabetic drugs to control blood sugar levels.
This treatment was ongoing for three months. Even after three months of regular dressing and controlled blood sugar levels, the ulcer was not healing. Later the patient was referred to our hospital to the plastic surgery department. Our hospital surgeon wanted a biopsy before planning any further management. An Edge wedge biopsy was sent to department of pathology for histo-pathological examination. Tissue was fixed in formalin overnight. Gross examination of lesion showed an irregular fragment of skin measuring 1×0.8×0.5cms. Cut surface showed blackish nodular area measuring 0.6×0.4×0.4cms, and was seen extending upto the resected surface. The resected surface was inked, specimen was bisected and all embedded in two blocks. Automated tissue processing was done and slides were reviewed microscopically. Microscopic examination revealed skin with an infiltrating malignant neoplasm with ulceration of overlying epithelium. The neoplastic cells arranged in nodular pattern. Cells vary in sizes and shape, are highly pleomorphic with irregular enlarged nuclei and prominent eosinophillic nucleoli. Numerous melanophages noted. The resected margin was involved by tumour cells. The case was diagnosed was Malignant melanoma, nodular type. Maximum tumour thickness was atleast 6mm since the resected margin was involved, definitve measurement would be possible on complete excision of specimen. Anatomic clark level was IV, melanoma invades reticular dermis. Subcutis was not represented in this biopsy to examine foe level V Mitotic grade – 3 per 10 High Power Field Microsatellite, lymphovascular invasion, neurotropism, tumour infiltrating lymphocytes, tumour regression – not identified in this biopsy Pathological staging was deferred to the definitive resection.
We immediately alerted the surgeon regarding the report. Following which patient was referred form department of plastic surgery to department to surgical oncology. Since the resected margin was positive, before directly proceeding with complete excision of tumour. Patient was subjected to further assessment to determine the clinical stage. A PET-CT was performed for this patient, which showed prominent external iliac nodal mass and popliteal nodes with significant pet uptake. Hence the modality of treatment suggested was Neo-adjuvant Immunotherapy.
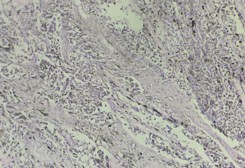
Fig (1): Hematoxylin and eosin stain, 100x. Infiltrating melanoma cells with ulceration of overlying epithelium.
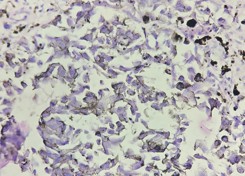
Fig (2): Hematoxylin and eosin stain, 400x. Neoplastic cells with karyomegaly and prominent nucleolus.
Discussion
Melanoma is an aggressive melanocytic neoplasm with a continuously increasing incidence worldwide and carries a poor prognosis. Nodular malignant melanoma usually occurs in chronically sun exposed areas. Histologically the vertical growth is more than the radial growth. Hence usually there is rapid growth with advanced Breslow depth, which is a poor prognostic factor. Nodular malignant melanoma is responsible for 40% of melanoma deaths. [3] The treatment of melanoma has been a challenge for several years due to its molecular heterogenicity. In recent years due to the rise of diagnostic molecular genetics, more specific targeted therapies were introduced. Hence the surveillance rate has increased in recent years and have renewed patient hope. Melanoma has historically been a formidable challenge in oncology, particularly in its advanced stages. The landscape of melanoma treatment has undergone a dramatic transformation in the past decade, largely due to the advent of immune-checkpoint inhibitors (ICIs) and targeted therapies [4] Testing for actionable mutations is recommended. Mutation testing of BRAF V600 is mandatory, whereas testing for other BRAF mutations is optional. Testing can be offered for NRAS and c-KIT mutations; testing for NTRK alterations is recommended in the absence of BRAF or RAS mutations. [5]
In addition to the mutational status, reporting programmed death-ligand 1 (PD-L1) expression by immunohistochemistry is recommended for all unresectable stage III and IV melanoma, since the European Medicines Agency (EMA) has approved the administration of nivolumaberelatlimab only in patients with tumour cell PD-L1 expression With the introduction of ICIs and targeted therapies (BRAF/MEK inhibitors), the treatment of advanced (unresectable or metastatic) cutaneous melanoma has been revolutionized. In fact, until the introduction of these agents, the median survival (mOS) of patients with advanced melanoma was about 6 months (Garbe et al., 2011). To date, 6-year mOS has been reached. [4]
Conclusion
Melanoma is distinct from nonmelanoma skin cancers because it spreads locally, regionally, and distantly. Invasive melanomas account for about 1% of all skin cancer cases, but they account for over 75% of skin cancer deaths [1]. Once a suspicious skin lesion is identified, a biopsy must be performed to confirm the diagnosis of melanoma. An excisional biopsy is the preferred biopsy modality. Melanoma treatment typically involves wide local excision, Mohs micrographic surgery, digital amputations, or adjuvant therapy depending on tumor location, depth, ulceration, lymph node involvement, and metastasis. Melanoma is the deadliest form of skin cancer. Therefore, early and correct diagnosis is key for ensuring patients have the best possible prognosis.
Acknowledgement: Dr. Anis B [Department of surgical oncology].
Reference
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023 Jan;73(1):17-48.
- Akbani, R., Akdemir, K.C., Aksoy, B.A., Albert, M., Ally, A., Amin, S.B., et al., 2015. Genomic classification of cutaneous melanoma.
- Smoller BR. Histologic criteria for diagnosing primary cutaneous malignant melanoma. Mod Pathol. 2006 Feb;19 Suppl 2: S34-40.
- Garbe, C., Eigentler, T.K., Keilholz, U., Hauschild, A., Kirkwood, J.M., 2011. Systematic review of medical treatment in melanoma: current status and future prospects. Oncologist 16, 5–24.
- Long, G.V., Atkinson, V., Lo, S., Guminski, A.D., Sandhu, S.K., Brown, M.P., et al., 2021. Five-year overall survival from the anti-PD1 brain collaboration (ABC Study): randomized phase 2 study of nivolumab (nivo) or nivo+ipilimumab (ipi) in patients (pts) with melanoma brain metastases (mets), 9508–9508 J. Clin. Oncol. 3
