Chordoid meningioma of the olfactory groove: A rare scent
Abstract
Background: Chordoid meningioma is a rare WHO grade 2 meningioma characterized by a lobulated, chordoma like pattern with a mucoid matrix. We present a 38 year old woman who presented extra axial dural based mass above the cribriform plate. Histopathological diagnosis was chordoid meningioma, CNS WHO grade 2. This case highlights the importance of integrating neuroimaging, histology, and immunohistochemistry to distinguish this rare, aggressive variant from histologic mimics and to guide postoperative management.
Key words: Chordoid meningioma; World Health Organization (WHO); Craniotomy
Introduction
Meningiomas are among the most common primary intracranial tumors, accounting for approximately 36% of all primary brain tumors. The World Health Organization (WHO) classifies meningiomas into three grades: grade 1 (benign), grade 2 (atypical), and grade 3 (anaplastic or malignant). Chordoid meningioma is a rare WHO grade 2 variants, constituting less than 0.5% of all meningiomas. It mimics chordoma or other chordoid pattern tumors. Chordoid meningiomas are associated with a more aggressive clinical course and higher recurrence rates, particularly when subtotal resection has been performed. [1]
Case Presentation
A 38-year-old woman presented to the outpatient department with a history of intermittent headaches of 3–4 months’ duration, associated with a mild reduction in sense of smell and occasional episodes of blurred vision. There was no history of seizures, focal weakness, or significant weight loss. On systemic examination, the cardiovascular, respiratory, and gastrointestinal systems were within normal limits. Neurological examination revealed intact cranial nerve function except for a reduced sense of smell; no focal neurological deficit was detected.
Routine hematological investigations revealed microcytic hypochromic anemia with neutrophilic leukocytosis. Biochemical profile, including renal and liver function tests, electrolytes, and viral markers, were within normal limits. Given the presence of localized neurological symptoms, hyposmia and visual blurring an MRI of the brain was performed. The MRI showed a large extra axial, dural based mass lesion measuring approximately 5.5 × 4 × 3 cm, located just above the cribriform plate and impinging on the frontal lobe. The lesion was iso intense to gray matter on both T1 and T2 weighted images, with avid post contrast enhancement and no evidence of surrounding brain parenchyma infiltration or calcification. A clinical diagnosis of meningioma was considered, and the patient underwent surgical excision via a craniotomy.
Gross examination of the excised specimen revealed multiple fragments ranging from 5 × 4 cm to 2 × 2 cm, with a gray, white, solid, partially congested cut surface. Microscopic examination showed tumor cells arranged in cords and nests within an abundant mucoproteinaceous background, with abundant cytoplasmic vacuolations producing a microcystic like appearance. (Fig 1) Mitotic activity was low (3 mitoses per 10 high power fields), without necrosis, marked cytological atypia, small cell component, or sheet like architecture. (Fig 2) Periodic acid–Schiff (PAS) stain was negative, whereas Alcian blue highlighted the myxoid matrix (Fig 3). Immunohistochemistry demonstrated occasional S100 positivity, diffuse moderate intensity progesterone receptor (PR) positivity, pancytokeratin (pan CK) negativity, and noncontributory epithelial membrane antigen (EMA) staining. The Ki 67 proliferation index was 7–8%. Based on these findings, the final diagnosis was chordoid meningioma, CNS WHO grade 2.
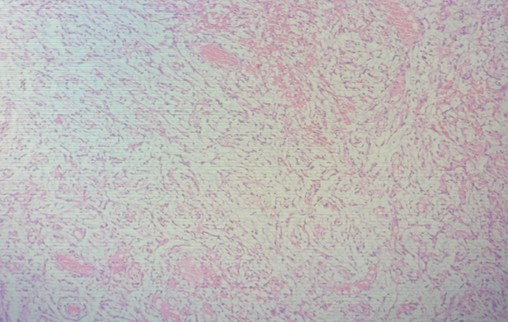
Fig (1): Section shows interconnecting cords of cells with scant cytoplasm and fine chromatin mixed with congestion and mucoid background. HE stains ×100
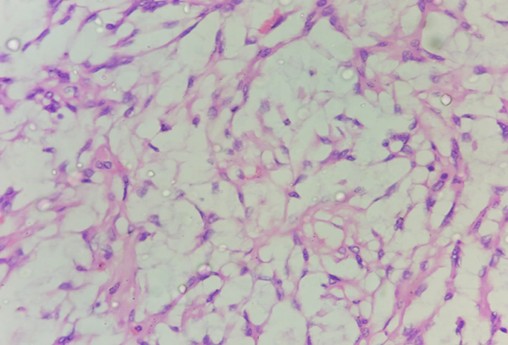
Fig (2): High power view of the tumor demonstrating microcystic appearance and cords of cells in a muco proteinaceous background. HE stains ×400
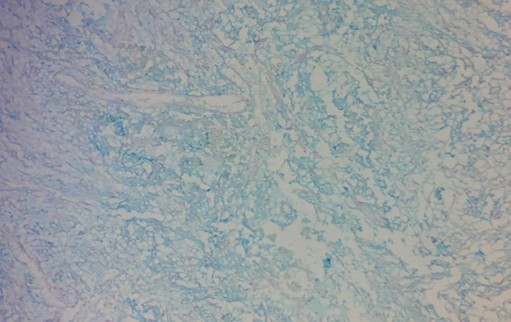
Fig (3): Alcian Blue stain highlights the myxoid matrix, AB stain×100
Discussion
Chordoid meningioma is a rare WHO grade 2 meningioma that typically occurs in adults, with a predilection for the skull base and convexity regions. [2] The lesion in our patient, located above the cribriform plate, is consistent with the anterior skull base localization reported in several case series. This anatomical location can produce symptoms such as headache, olfactory dysfunction, and visual disturbances due to impingement on the frontal lobe and adjacent optic structures.
Radiologically, chordoid meningiomas often show facilitated diffusion on MRI, with higher ADC values compared with other meningioma subtypes. [3] The absence of calcification in the present case is also consistent with the typical MRI features of chordoid meningioma. Due to their aggressive behavior and higher recurrence rates, complete surgical resection is the primary goal, and adjuvant radiotherapy may be considered, especially in cases with subtotal resection or aggressive features.
Histologically, chordoid meningioma is characterized by cords and nests of epithelioid cells embedded in a myxoid matrix, which stains positive with Alcian blue and may resemble chordoma or other chordoid pattern tumors.[4] The focal S100 positivity observed in our case is consistent with prior reports, where S100 may be present in a minority of cells; however, brachyury negativity would be required to exclude chordoma.
In chordoid meningioma, EMA and PR are typically positive, whereas pan CK is negative, which aligns with the immunohistochemical profile in our case. The Ki 67 proliferation index of 7–8% is within the range reported for this grade 2 variant and supports its intermediate biological behavior. [5,6,7]
Conclusion
Chordoid meningioma is a rare WHO grade 2 meningioma with a chordoma like histologic pattern and myxoid matrix. [1] The present case highlights the importance of integrating clinical presentation, neuroimaging, histopathology, and immunohistochemistry to establish a definitive diagnosis and differentiate this variant from chordoma and other chordoid pattern tumors. Complete surgical excision is essential, and long term follow up is recommended due to the increased risk of recurrence associated with this aggressive subtype.
References
- Prokopienko M, et al. Chordoid meningioma: Case report and review of literature. Cureus. 2022.
- Jie D, et al. Clinical features, radiological findings, and prognostic factors of chordoid meningioma. Front Neurol. 2022.
- Radiation reference article on chordoid meningioma. Radiopaedia. 2024.
- Misdiagnosis of chordoma: A case report and review of literature. Medicine. 2025.
- Distinguishing chordoid meningiomas from their histologic mimics. Mod Pathol. 1997.
- Chordoid meningioma: Differentiating a rare WHO grade II meningioma on MRI. AJNR. 2015.
- A short series of chordoid meningioma cases. Austin J Neurosurg.
