Pulmonary melioidosis in a poorly controlled diabetic: A case report
Abstract
Background: Melioidosis, caused by Burkholderia pseudomallei, is an emerging infection in Southeast Asia and India, with diabetes mellitus as the most significant risk factor. The disease often mimics tuberculosis or community-acquired pneumonia, leading to delayed diagnosis.
Case presentation: A 53-year-old male with poorly controlled diabetes presented with fever, cough, dyspnoea, and reduced oral intake for 10 days. Despite treatment in two other hospitals, his symptoms persisted. Chest radiograph showed right lower lobe consolidation with multilocular effusion. Pleural fluid culture grew B. pseudomallei. The patient was successfully treated with intravenous ceftazidime and oral trimethoprim–sulfamethoxazole, followed by eradication therapy. Follow-up demonstrated 95% clinical and radiological resolution.
Conclusion: This case highlights the importance of considering melioidosis in diabetic patients with non-resolving pneumonia and underscores the role of microbiological confirmation for timely treatment.
Key words: Melioidosis; Burkholderia pseudomallei; Eradication therapy.
Introduction
Melioidosis is an infection caused by the Gram-negative bacilli Burkholderia pseudomallei. The disease is endemic to Southeast Asia and northern Australia, with an increasing number of cases being reported in India. Clinical presentation is highly variable, ranging from localized skin infection to severe pneumonia and septicemia. Diabetes mellitus is the strongest risk factor, reported in more than 50% of cases. Misdiagnosis as tuberculosis or bacterial pneumonia is common, leading to inappropriate therapy and high mortality.
Case Presentation
A 53-year-old male, known diabetic with poor glycaemic control, presented with fever, cough, dyspnoea, and reduced oral intake for 10 days. He had been treated empirically in two other hospitals with no resolution of symptoms.
On admission
| Pulse | 91/min |
| Blood pressure | 140/80 mmHg |
| Sp O₂ | 91% on room air |
| Cardiovascular system | S1, S2 normal |
| Respiratory system | Bronchial breath sounds in right lower lung zone |
Investigations
| Chest radiograph | Right lower lobe consolidation with multilocular effusion. |
| Pleural fluid analysis | Exudative fluid. |
| Culture | Pleural fluid inoculated in rapid blood culture bottles, showing growth of Gram-negative bacilli within 24 hours. Subculture on MacConkey agar revealed wrinkled, dry, non-lactose fermenting colonies. |
| Gram stain | Demonstrated Gram-negative bacilli with bipolar (“safety-pin”) staining. |
| Biochemical identification | Oxidase positive; resistant to aminoglycosides and colistin; confirmed as Burkholderia pseudomallei using Vitek 2 system. |
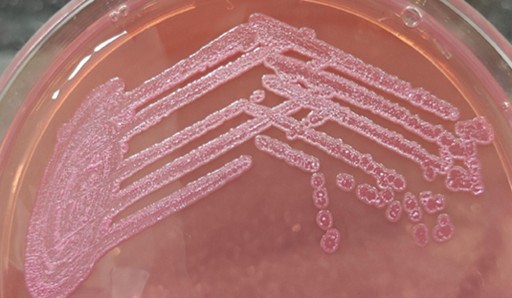
Fig (1): Colony morphology of B. pseudomallei on MacConkey agar, showing wrinkled, dry, non-lactose fermenting colonies
Treatment
- Intensive phase: Intravenous ceftazidime (2 g twice daily) plus oral trimethoprim–sulfamethoxazole with folic acid supplementation.
- Eradication phase: Oral trimethoprim–sulfamethoxazole every 12 hours with folic acid for 3–6 months to prevent relapse.
Outcome and Follow-up
The patient improved within one week and was discharged in stable condition. At follow-up after two weeks, he reported 95% resolution of symptoms with radiological improvement. He continues eradication therapy.He is currently on eradication phase of treatment.
Discussion
Melioidosis is increasingly reported in India but remains under-recognized. The first indigenous case from India was detected in Mumbai in 1991. The high prevalence of diabetes, combined with factors such as state-wise average annual rainfall and widespread paddy cultivation, creates an environment conducive to the growth of B. pseudomallei. Given these factors, India has a high potential to become an endemic country for the disease, underscoring the urgent need for increased awareness, surveillance, and research to mitigate the growing public health threat it presents. Due to improvement in diagnostic facilities has led to identification of more cases of melioidosis, along the coastal regions from the states of Karnataka, Kerala, and Tamil Nadu. Despite the growing recognition of melioidosis, there is still no formal surveillance for the disease in South Asia, particularly in India, where it is often misdiagnosed as tuberculosis or common pneumonia. We have reported 30 cases of Burkholderia pseudomallei within the past 5 years in our Centre. Pulmonary involvement is the most common presentation and may mimic tuberculosis, community-acquired pneumonia, or lung abscess. As per CDC Melioidosis 2023 case definition, our patient can be categorized under confirmed case category.
Microbiological perspective
- Culture remains the gold standard for diagnosis. While culture based techniques are gold standard, their sensitivity can be variable depending on the type of specimen and bacterial load. Whenever there is high clinical suspicion, it is advisable to inoculate the sample in automated aerobic blood culture bottles thereby increasing the sensitivity.
- Gram stain may show the typical bipolar “safety-pin” appearance.
- On MacConkey agar, B. pseudomallei produces dry, wrinkled, non-lactose fermenting colonies.
- The organism is oxidase positive, intrinsically resistant to aminoglycosides and colistin, but sensitive to ceftazidime, meropenem, and co-trimoxazole. While acquired resistance is rare, there are few reports that have reported resistance to ceftazidime. In a study done by Suseela et al, out of a total of 73 isolates, 2 cases were resistant to ceftazidime (2.7%).
- Misidentification as Pseudomonas is possible, emphasizing the need for high suspicion in endemic regions.
Treatment approach
A two-phase regimen is essential. Ceftazidime or meropenem forms the backbone of intensive therapy, followed by prolonged oral eradication with trimethoprim–sulfamethoxazole to prevent relapse.
The mortality rate for acute melioidosis ranges up to 90%, although it mainly varies from 20 to 50% in different settings globally. Good clinical clues, early diagnosis, appropriate use of antibiotics, and comorbidities all contribute to the outcome of the disease.
Learning Points
- Consider melioidosis in diabetic patients presenting with non-resolving pneumonia in endemic areas.
- Culture confirmation is essential, with characteristic Gram stain and MacConkey agar features aiding rapid recognition.
- A two-phase treatment regimen (intensive IV + prolonged oral eradication) is mandatory to prevent relapse.
References
- Cheng AC, Currie BJ. Melioidosis: epidemiology, pathophysiology, and management. Clin Microbiol Rev. 2005;18(2):383–416.
- Dance DAB. Treatment and prophylaxis of melioidosis. Int J Antimicrob Agents. 2014;43(4):310–318.
- Limmathurotsakul D, et al. Melioidosis: a clinical overview. Trop Med Infect Dis. 2018;3(1):38.
- Kannan S, Singh S, Earny VA, Chowdhury S, Ashiq M, Eshwara VK, Mukhopadhyay C, Kaur H. Two Decades of Melioidosis in India: A Comprehensive Epidemiological Review. Pathogens. 2025 Apr 14;14(4):379. doi: 10.3390/pathogens14040379. PMID: 40333168; PMCID: PMC12030058.
- National Centre for Disease Control (NCDC).CD alert – Melioidosis. Directorate of Health Services, Govt. of India. April 2019. https://ncdc.mohfw.gov.in/wp-content/uploads/2024/10/Revised-CD-Alert-Mpox-1.pdf.
- Mohapatra PR, Behera B, Mishra B. Melioidosis: An Indian Perspective. J Assoc Physicians India 2025;73(5):63-68.
- Suseela, Kundoly Velayudhan; Alex, Aiswariya; Das, Subi. Clinical Presentations of Melioidosis and Antibiogram of Burkholderia pseudomallei: An 8-year Study in a Tertiary Care Center, South India. International Journal of Advanced Medical and Health Research 11(1): p 31-35, Jan–Jun 2024. | DOI: 10.4103/ijamr.ijamr_123_23.
- Centers for Disease Control and Prevention. Melioidosis (Burkholderia pseudomallei) 2023 Case Definition. https://ndc.services.cdc.gov/case-definitions/melioidosis-burkholderia-pseudomallei-2023/. Published February 28, 2023.
