Comprehensive audit of TB diagnostic utilization and yield in a tertiary care hospital, Trichy
Abstract
Background: Accurate and prompt diagnosis is critical for tuberculosis (TB) control. Despite advancements, reliance on insensitive methods and delays in drug-resistant TB (DR-TB) detection remain major obstacles to achieving global End TB targets. Despite the recovery of health services post-COVID, a significant “diagnostic gap” persists; approximately 2.7 to 3.6 million people with TB are either undiagnosed or not officially reported to health authorities annually. This gap is a primary driver of ongoing community transmission. This audit examines the alignment between laboratory practice and policy, specifically identifying discrepancies in the uptake of molecular testing and the reporting of drug-resistant TB cases.”
Key words: Drug-resistant TB (DR-TB); Ziehl–Neelsen (ZN) staining technique; Real-time polymerase chain reaction (RT-PCR)
Aim
- To evaluate appropriateness, timeliness, and accuracy of TB diagnostic testing
- To assess utilization of Smear, molecular tests and Culture for TB diagnosis
- To identify gaps in DR-TB detection and reporting
Audit Period: September 2024–August 2025
Audit Population: All patients who were tested for Tuberculosis (TB) during the defined audit period were included in the analysis.
Exclusion Criteria: Repeated samples from same patients were excluded from this study.
Test Methodology
AFB Smear Microscopy: Performed using the Ziehl–Neelsen (ZN) staining technique for detection of acid-fast bacilli under light microscopy.
TB PCR (Molecular Testing): Conducted using real-time polymerase chain reaction (RT-PCR) for qualitative detection of Mycobacterium tuberculosis complex, along with simultaneous assessment of rifampicin resistance.
Mycobacterial Culture: Performed using the Mycobacteria Growth Indicator Tube (MGIT) system, a liquid culture method for isolation of mycobacteria and further confirmation.
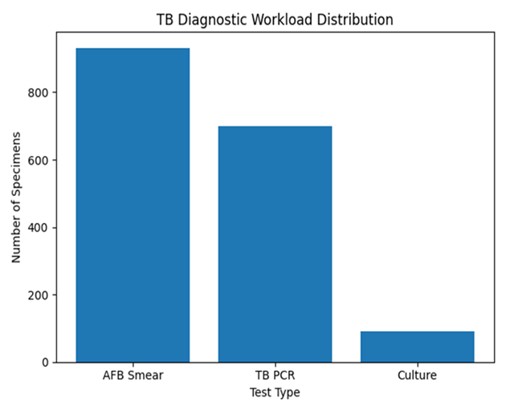
TB Diagnostic Workload Distribution
Overall samples received for TB Testing :1200
| Test Type | Number of Specimens | Percentage (%) |
|---|---|---|
| AFB Smear | 932 | 77.6% |
| TB PCR | 699 | 58.2% |
| Culture | 91 | 7.5% |
| Test Requested | Number of Cases | Percentage |
|---|---|---|
| AFB smear only | 489/1200 | 40.7% |
| TB PCR only | 256/1200 | 21.3% |
| AFB smear + TB PCR | 443/1200 | 36.9% |
| TB culture (total) | 91/1200 | 7.6% |
| Culture only | 12/1200 | 1.0% |
- AFB smear alone was the most frequently ordered test (40.7%).
- Combined testing (smear + PCR) was performed in 36.9% of cases, improving diagnostic correlation.
- PCR alone accounted for 21.3%, reflecting increasing use of molecular diagnostics.
- Culture was performed in 7.6% of cases, mainly along with other tests.
- Culture alone was rarely requested (1%).
AFB Smear Utilization
| Category | Number | Percentage |
|---|---|---|
| AFB smear only | 489 | 52.5% |
| AFB smear + other tests (PCR /culture) | 443 | 47.5% |
| Total AFB smear specimens | 932 | 100% |
Specimen-wise Distribution in AFB Smear Only Cases (489)
| Specimen | Cases | Percentage |
|---|---|---|
| Sputum | 236 | 48.3% |
| Pus | 94 | 19.2% |
| CSF | 42 | 8.6% |
| Tracheal | 37 | 7.6% |
| BAL | 21 | 4.3% |
| Tissue | 23 | 4.7% |
| Body fluids | 19 | 3.8% |
| FNA slide | 14 | 2.9% |
| Urine | 3 | 0.6% |
- Among AFB smear-only requests, Respiratory specimen constituted the majority (around 60%)
- However, a significant proportion of extrapulmonary and paucibacillary specimens were also tested by smear alone, where molecular methods could improve diagnostic yield.
- Only 47% of samples had additional tests such as TB PCR or culture.
Limitations of AFB Smear-Only Testing:
Inherent Limitation of Smear Microscopy
AFB smear requires a high bacillary load (~10⁴ bacilli/mL) for detection. As a result, smear-only testing has poor sensitivity in
- Smear-negative pulmonary TB
- Extrapulmonary TB (EPTB)
- Pediatric TB
- People living with HIV (PLHIV)
This significantly increases the risk of missed or delayed diagnosis in clinically important subgroups.
Extremely Low Positivity Rate (1.6%)
Out of all AFB smear samples, only 8 cases (1.6%) were positive. This indicates either low bacillary burden in the tested population, or Limited diagnostic yield of smear microscopy alone. This highlights the need for more sensitive diagnostic modalities like PCR.
Inability to Differentiate MTB vs NTM
A major limitation of smear microscopy is it Cannot distinguish Mycobacterium tuberculosis (MTB) from Non-Tuberculous Mycobacteria (NTM) . This has significant clinical implications, as management differs completely.
Diagnostic Uncertainty in Smear-Positive Cases
Among the 8 smear-positive cases, 2 cases were clinically suspected NTM infections, 6 cases remained undifferentiated (MTB vs NTM). This creates a diagnostic ambiguity, potentially leading to Inappropriate anti-TB treatment, Delay in correct diagnosis (especially NTM cases) and Impact on patient outcomes and antimicrobial stewardship.
Overall TB PCR Analysis
| Parameter | Value |
|---|---|
| Overall samples tested by TB PCR | 699 |
| TB PCR positive | 97 |
| TB PCR negative | 602 |
| Positivity rate | 14% |
The TB PCR analysis over the audit period demonstrates a moderate diagnostic yield, with 97 out of 699 samples testing positive, resulting in a positivity rate of 14% (approximately 1 in 7 samples). This suggests reasonably appropriate clinical selection of cases for molecular testing and reflects a good pre-test probability in the evaluated population. The use of PCR has clearly enhanced diagnostic capability compared to smear microscopy, particularly in detecting paucibacillary cases such as smear-negative pulmonary TB, extrapulmonary TB, pediatric TB, and HIV-associated TB, thereby enabling earlier and more accurate diagnosis. However, the high proportion of negative results (86%) indicates the need to further evaluate clinical selection criteria and sample quality, as some cases may represent either true negatives or missed diagnoses due to low bacillary load or suboptimal specimens.
Specimen wise positivity rate
| Specimen Type | Positivity (%). |
|---|---|
| Sputum | 39% |
| Bronchoalveolar Lavage (BAL) | 28% |
| Pus / Tissue | 19% |
| Body Fluid Samples | 7% |
| Endotracheal (ET) Sam-ple | 4% |
| Urine | 2% |
| Bone Marrow | 0.5% |
Specimen-wise analysis shows that respiratory samples yield the highest positivity, with sputum (39%) and bronchoalveolar lavage (28%) contributing significantly to case detection, highlighting effective targeting of pulmonary TB. Moderate positivity in pus and tissue samples (19%) reflects the value of PCR in extrapulmonary TB diagnosis, especially when adequate samples are obtained. In contrast, body fluids (7%), urine (2%), and bone marrow (0.5%) show low positivity rates, likely due to the paucibacillary nature of these specimens, emphasizing the importance of clinical correlation and the need for adjunct diagnostic methods.
TB PCR Positive Bacillary Load Distribution
| Bacillary Load | Cases |
|---|---|
| High | 13 |
| Medium | 26 |
| Low | 38 |
| Very Low | 20 |
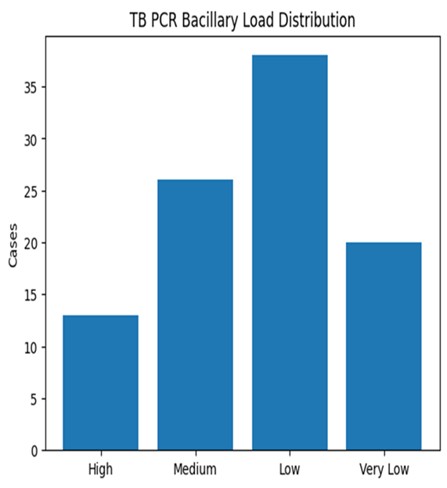
The distribution of bacillary load among TB PCR–positive cases shows that the majority of patients fall within the low to very low bacillary burden categories, with 38 cases classified as low and 20 as very low, together accounting for a significant proportion of detected cases. In contrast, only 26 cases had medium bacillary load, and 13 cases had high bacillary load. This pattern highlights an important clinical insight: a large proportion of TB cases in this cohort are paucibacillary, which would likely have been missed by conventional smear microscopy due to its higher detection threshold.
The predominance of low bacillary load cases underscores the critical role of molecular diagnostics (TB PCR) in early and accurate detection, particularly in patient groups such as extrapulmonary TB, pediatric patients, and immunocompromised individuals (including HIV), where bacillary burden is typically low. At the same time, the relatively smaller proportion of high bacillary load cases suggests that fewer patients are presented at advanced, highly infectious stages, which may reflect earlier testing or clinical suspicion.
From an audit perspective, this distribution reinforces that reliance on smear microscopy alone would lead to significant underdiagnosis, whereas PCR enables identification across the full spectrum of disease burden. However, it also highlights the need for careful clinical correlation, especially in very low bacillary load cases, where the risk of false positives or detection of non-viable organisms may exist. Overall, these findings strongly support the integration of PCR as a primary diagnostic tool, complemented by culture where necessary for confirmation and drug susceptibility testing.
Rifampicin Resistance in TB PCR Positive Cases
| Rifampicin Resistance | Cases |
|---|---|
| Not Detected | 72 |
| Indeterminate | 24 |
| Detected | 1 |
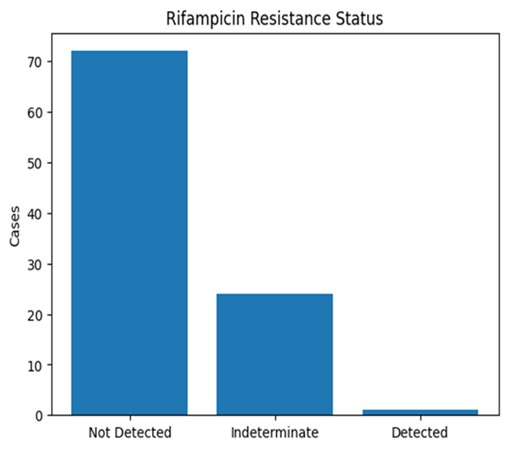
The analysis of rifampicin resistance among TB PCR–positive cases shows that 72 cases were reported as “Not Detected,” 24 as “Indeterminate,” and only 1 case as “Detected.” This indicates that the majority of confirmed TB cases in this cohort are likely rifampicin-sensitive, which is a reassuring finding from both a treatment and public health perspective, suggesting a relatively low burden of drug-resistant TB in the tested population.
However, a key concern in this dataset is the high proportion of indeterminate results (24 out of 97 cases, ~25%). Indeterminate rifampicin resistance is often associated with low or very low bacillary load, suboptimal sample quality, or technical limitations of the assay. This aligns with the earlier findings that a large proportion of cases have low bacillary burden, which can reduce the assay’s ability to reliably detect resistance mutations. From an audit standpoint, this represents a significant diagnostic gap, as these patients fall into an uncertain category where appropriate treatment decisions may be delayed.
The single detected rifampicin-resistant case (~1%) suggests a low prevalence of probable multidrug-resistant TB (MDR-TB) in this setting. While this is encouraging, it should be interpreted cautiously, given the limited use of culture and drug susceptibility testing (DST) in overall diagnostic workflow. There remains a possibility of under-detection of drug resistance, especially in cases not subjected to confirmatory testing.
Clinically, these findings emphasize the importance of follow-up testing for indeterminate results, including repeat PCR with better-quality samples or culture-based DST where feasible. Strengthening sample collection techniques and ensuring adequate specimen volume can help reduce indeterminate outcomes. Additionally, integrating a protocol for mandatory reflex testing in all indeterminate cases will improve diagnostic clarity and guide appropriate therapy.
In conclusion, while rifampicin resistance appears low in this cohort, the high indeterminate rate is a critical audit finding that needs targeted intervention. Addressing this gap will enhance the reliability of resistance detection and support better TB management and antimicrobial stewardship.
TB PCR Only Cases (256)
| TB PCR Only Result | Cases |
|---|---|
| Detected | 23 (9.8%) |
| Not Detected | 233 |
Disadvantages of using only TB PCR:
Among the 256 TB PCR-only cases, 23 (9.8%) were detected as positive while the majority, 233 cases, were negative, indicating a relatively low diagnostic yield when PCR is used as a standalone test. Although TB PCR is a rapid and sensitive molecular tool, relying on it alone has several important limitations. It may miss certain paucibacillary and extrapulmonary TB cases, particularly when bacillary load is extremely low or sample quality is suboptimal. Additionally, TB PCR is designed to detect Mycobacterium tuberculosis complex and therefore cannot identify non-tuberculous mycobacteria (NTM), leading to potential misclassification in clinically suspected cases. Another critical limitation is that PCR cannot replace culture, which remains essential for definitive confirmation and comprehensive drug susceptibility testing (DST), especially in the context of emerging drug-resistant TB.
It is also important to note that PCR positivity does not always indicate the presence of viable bacilli, particularly in cases with very low bacillary load in respiratory specimens, where residual or non-viable DNA may be detected. Overall, while TB PCR is highly valuable for rapid diagnosis, these findings highlight that PCR should be integrated with smear microscopy, culture, and clinical correlation, rather than being used in isolation, to ensure accurate diagnosis and optimal patient management.
Four-Quadrant Table: AFB Smear vs TB PCR
| Name | TB PCR Detected | TB PCR Not Detected | Total |
|---|---|---|---|
| AFB Smear Positive | 50 | 3 | 53 |
| AFB Smear Negative | 24 | 366 | 390 |
| Total | 74 | 369 | 443 |
The four-quadrant comparison between AFB smear and TB PCR demonstrates important diagnostic differences and reinforces the limitations of smear microscopy. Among the 443 cases analyzed, 50 cases were positive by both smear and PCR, while 365 cases were negative by both methods, showing overall agreement in a majority of cases. However, a key finding is that 24 cases were smear-negative but PCR-positive, highlighting the superior sensitivity of PCR in detecting paucibacillary disease, particularly in low and very low bacillary load categories. This confirms that reliance on smear alone would have resulted in missed TB diagnoses in a significant number of patients.
Conversely, there were 3 cases that were smear-positive but PCR-negative, which is clinically significant. Further evaluation revealed that 3 of these cases were due to non-tuberculous mycobacterial (NTM) infections, organisms that can appear acid-fast on smear but are not detected by TB PCR. This finding underscores a critical limitation of smear microscopy—its lack of specificity, as it cannot differentiate Mycobacterium tuberculosis from other acid-fast organisms.
Overall, this analysis clearly demonstrates that TB PCR provides higher sensitivity and better specificity compared to smear microscopy, particularly in detecting true TB cases and avoiding misclassification of non- tubercular infections. It strongly supports the need for integrated diagnostic approaches, where smear findings are confirmed with PCR, and discrepant cases are further evaluated with culture or additional tests, to ensure accurate diagnosis and appropriate patient management.
AFB Culture Results (91)
| Culture Result | Number of Cases | Percentage |
|---|---|---|
| Mycobacterium tu-berculosis detected | 15 | 16.5% |
| NTM detected | 1 | 1.1% |
| Culture negative | 75 | 82.4% |
| Total | 91 | 100% |
Culture Utilization Pattern
| Test Combination | Number of Cases |
|---|---|
| Culture only requested | 12 |
| Culture with other tests (AFB smear / TB PCR) | 79 |
The analysis of AFB culture results (n=91) shows that Mycobacterium tuberculosis was detected in 15 cases (16.5%), while 1 case (1.1%) grew non-tuberculous mycobacteria (NTM), and the majority, 75 cases (82.4%), were culture negative. This indicates a modest diagnostic yield of culture, which may be influenced by factors such as prior antibiotic exposure, low bacillary load, or sample quality. Despite its lower positivity rate, culture remains the gold standard for TB diagnosis, particularly because it enables definitive confirmation, differentiation of MTB from NTM, and drug susceptibility testing (DST)all of which are critical for appropriate patient management and detection of drug-resistant TB.
The culture utilization pattern reveals that 79 out of 91 cases were performed in combination with other tests (smear and/or PCR), while only 12 cases had culture requested as a standalone test. This suggests that clinicians generally prefer a combined diagnostic approach, which is appropriate. However, it is noteworthy that among these 12 culture-only cases, 11 were extrapulmonary samples, where TB is often paucibacillary and difficult to diagnose. In such cases, the absence of adjunct molecular testing likely reduced the diagnostic yield, and the addition of TB PCR could have significantly improved early detection.
From an audit perspective, a key concern is that culture remains underutilized overall, despite its critical role in confirming diagnosis and guiding therapy. The high proportion of culture-negative results, combined with limited standalone use, highlights the need to optimize test selection and ensure appropriate combination with molecular methods. Strengthening protocols to include PCR alongside culture, especially in extrapulmonary and high-risk cases, would improve diagnostic accuracy. Overall, while culture is being used appropriately in combination settings, its expanded and more strategic utilization is essential for comprehensive TB diagnosis, NTM identification, and effective drug resistance surveillance.
TB PCR positive, AFB culture negative Specimens
| TB PCR Detection Lev-el | Number of Samples |
|---|---|
| Very low detected | 5 |
| Low detected | 1 |
| Medium detected | 1 |
The subset of TB PCR–positive but AFB culture–negative specimens (n=7) provide an important insight into the added value of molecular diagnostics. Among these cases, 5 showed very low detection, 1 low, and 1 medium bacillary load, indicating that the majority were paucibacillary in nature. This explains the negative culture results, as culture sensitivity is often reduced in samples with very low organism burden or in patients who may have received prior treatment.
From an audit perspective, this finding highlights that TB PCR significantly enhances case detection beyond conventional methods, particularly in cases that would otherwise be missed by both smear microscopy and culture. The ability of PCR to detect minimal quantities of mycobacterial DNA makes it especially valuable in extrapulmonary TB, early disease, and immunocompromised patients, where bacillary load is typically low.
However, these results should also be interpreted with caution. PCR positivity in very low bacillary load cases may sometimes represent non-viable organisms or residual DNA, especially in previously treated patients. Therefore, clinical correlation is essential before initiating or continuing therapy.
Overall, this analysis reinforces that TB PCR is a critical complementary tool, improving diagnostic sensitivity and enabling earlier detection of probable TB cases, particularly when traditional methods such as culture yield negative results.
Summary
This clinical audit of TB diagnostics (September 2024 – August 2025) highlights important trends in current laboratory practices and provides an opportunity to benchmark them against recommendations from the National Tuberculosis Elimination Programme (NTEP) and the World Health Organization (WHO) [1,3]. Both agencies strongly advocate for a shift from conventional microscopy to rapid molecular diagnostics as the initial test for TB detection [2,4].
A key finding in this audit is the continued high reliance on AFB smear microscopy, with a significant proportion of patients undergoing smear-only testing. As per WHO and NTEP guidelines, smear microscopy should not be used as a standalone diagnostic tool due to its low sensitivity, particularly in paucibacillary conditions such as extrapulmonary TB, pediatric TB, and TB in people living with HIV [2]. This is reflected in the audit by the very low smear positivity rate (1.6%), confirming its limited diagnostic yield. Additionally, smear microscopy lacks specificity, as it cannot differentiate Mycobacterium tuberculosis from other acid-fast organisms, leading to potential misclassification such as NTM and, a limitation well recognized in existing literature [6,7].
In contrast, TB PCR (molecular testing) demonstrated a higher diagnostic utility, with a positivity rate of 14%, and a large proportion of cases in low and very low bacillary load categories. This aligns with WHO recommendations that molecular assays should be used as the initial diagnostic test in all suspected TB cases [2,4]. The audit findings further support this, as PCR identified smear-negative TB cases and additional probable TB cases among culture-negative samples, highlighting its superior sensitivity [5,6].
However, the audit also reveals areas for improvement. The high proportion of PCR-negative results (86%) suggests the need for better clinical selection and sample quality optimization, as emphasized in WHO frameworks [2]. Additionally, the high proportion of indeterminate rifampicin resistance results (~25%) is concerning and may be related to low bacillary load. WHO guidelines recommend that such cases undergo repeat testing or culture-based drug susceptibility testing (DST) for confirmation [2,8].
A critical gap identified is the underutilization of culture, despite its role as the gold standard for TB diagnosis. Culture is essential for confirmation and differentiation.
of MTB from NTM, and comprehensive drug susceptibility testing, as highlighted in both WHO and NTEP guidelines [2,3]. Limited culture use in this audit restricts the ability to detect drug-resistant TB, which is a key priority in TB control programs .[9]
The bacillary load distribution observed in this audit, with a predominance of low and very low bacillary burden cases, further supports WHO’s emphasis on molecular diagnostics, as these cases are frequently missed by smear microscopy . Additionally, PCR-positive but culture-negative cases demonstrate the enhanced sensitivity of molecular methods, particularly in early or paucibacillary disease .[5]
In summary, this audit demonstrates partial alignment with NTEP and WHO guidelines, particularly in the adoption of molecular diagnostics. However, significant gaps remain, including over-reliance on smear microscopy, underutilization of culture, and lack of standardized diagnostic algorithms. Strengthening PCR as the first-line test, implementing reflex testing protocols, and improving culture utilization are essential steps to align with global best practices and improve TB diagnosis and control outcomes .[2]
Limitations of the Clinical Audit (Study Drawbacks)
This clinical audit, while providing valuable insights into TB diagnostic practices, has certain limitations that should be considered when interpreting the findings. Firstly, the analysis is based purely on laboratory diagnostic data, without integration of clinical diagnosis or patient outcomes. As a result, the correlation between laboratory results and actual disease status could not be fully established, limiting the ability to assess true diagnostic accuracy.
Secondly, there was no incorporation of histopathological, cytological, or radiological findings, which are particularly important in the diagnosis of extrapulmonary and paucibacillary TB. The absence of these complementary modalities restricts a comprehensive evaluation and may lead to under- or overestimation of diagnostic performance, especially in cases where microbiological confirmation is challenging.
Another significant limitation is the unequal utilization of diagnostic tests. The audit demonstrates a high volume of AFB smear testing compared to relatively low use of culture, despite culture being the gold standard. This imbalance introduces a bias in comparative analysis, making it difficult to draw fully reliable conclusions regarding the relative performance of different diagnostic modalities. Additionally, inconsistent use of combined testing (smear, PCR, and culture) further limits the ability to standardize comparisons across patient groups.
Overall, these limitations highlight the need for a more integrated, multidisciplinary approach in future audits, incorporating clinical, radiological, and pathological data along with standardized diagnostic protocols to achieve a more accurate and balanced assessment of TB diagnosis.
References
- World Health Organization. Global tuberculosis report 2023. Geneva: World Health Organization; 2023.
- World Health Organization. WHO consolidated guidelines on tuberculosis. Module 3: Diagnosis – rapid diagnostics for tuberculosis detection. Geneva: WHO; 2021.
- Central TB Division. National Tuberculosis Elimination Programme (NTEP): Technical and Operational Guidelines for TB Control in India 2020. New Delhi: Ministry of Health and Family Welfare; 2020.
- World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/RIF assay. WHO policy statement; 2013.
- Steingart KR, Sohn H, Schiller I, et al. Xpert MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev. 2014;(1):CD009593.
- Pai M, Schito M. Tuberculosis diagnostics in 2015: landscape, priorities, needs, and prospects. J Infect Dis. 2015;211(S2):S21–S28.
- Perkins MD, Cunningham J. Facing the crisis: improving the diagnosis of tuberculosis in the HIV era. J Infect Dis. 2007;196(S1):S15–S27.
- World Health Organization. Guidelines for treatment of drug-susceptible tuberculosis and patient care. Geneva: WHO; 2017.
