Polymeric IgA mimicking biclonal gammopathy in relapsed IgA λ multiple myeloma: A case report
Abstract
Background: Monoclonal gammopathies (MGs) are typified by a clonal immunoglobulin (M protein) produced by plasma or lymphoplasmacytic cells. The usual electrophoretic pattern is a single sharp band in the gamma region. Occasionally, two distinct bands are observed, suggesting biclonal gammopathy. However, in certain instances, polymerisation of immunoglobulins especially IgA may result in distinct migration patterns, mimicking biclonality
Case presentation: We report a 66-year old male with known IgA lambda (λ) multiple myeloma who presented with relapse post autologous stem cell transplant (ASCT) and maintenance therapy. Serum protein electrophoresis (SPEP) revealed two monoclonal bands (β2 globulin region + γ globulin region; combined 1.26 g/dL). Immunotyping showed a broad polymeric IgA band with a single lambda light chain band. Following chemical reduction of serum with β mercaptoethanol (BME), repeat electrophoresis/immunofixation collapsed the two bands into a single sharp IgA λ peak migrating in the β2 region. Free light chains revealed a highly elevated λ chain (6,188 mg/L) with κ/λ ratio of 0.002, confirming relapse.
Conclusions: This case underscores the importance of considering IgA polymerisation when dual bands appear on SPEP, and demonstrates the utility of BME reduction to distinguish true biclonality from polymeric artefact. Accurate identification prevents misinterpretation of disease burden and ensures appropriate management in relapsed plasma cell dyscrasia.
Keywords: IgA polymerisation; Biclonal gammopathy; Multiple myeloma relapse; β Mercaptoethanol reduction; Serum protein electrophoresis
Introduction
Monoclonal gammopathies (MGs) comprise a spectrum of disorders characterized by clonal expansion of plasma or lymphoplasmacytic cells that produce excessive monoclonal immunoglobulins (Igs) — intact molecules or fragments (free light chains, truncated heavy chains) [1]. Typically, the M protein appears as a single narrow “spike” on serum protein electrophoresis (SPEP), commonly in the gamma region [2]. However, in some cases two distinct monoclonal bands emerge, raising the possibility of biclonal gammopathy — i.e., two independent M proteins, either from separate clones or from a single clone with dual isotype expression [3]. Alternatively, polymerization of certain isotypes (notably IgA) may produce multiple migrating forms of the same monoclonal protein, mimicking biclonality. This distinction is clinically important because management, prognosis and monitoring differ between true biclonal disease and polymeric artefact [4]. Chemical reduction with agents such as β mercaptoethanol (BME) can disrupt Ig polymers, collapsing multiple bands into a single band and clarifying clonality [5]. In this case, we report a patient with known IgA λ multiple myeloma at relapse whose apparent biclonal pattern was clarified by BME treatment.
Case Presentation
A 66-year-old male with known diagnosis of IgA lambda multiple myeloma initially treated with CyBorD (bortezomib, cyclophosphamide, dexamethasone) achieved a very good partial response (VGPR). Autologous stem cell transplantation (ASCT) was recommended but delayed as per patient preference; eventually he underwent ASCT and was maintained on bortezomib + lenalidomide (VR) therapy.
Several months post ASCT the patient developed decreased appetite, fatigue, nausea and fever, plus burning micturition. Urinalysis showed 8 10 pus cells; urine culture was sterile. Empirical antibiotic therapy was given, but fever persisted. Serum procalcitonin was within normal limits. He then developed progressive dyspnea, tachycardia and hypoxaemia requiring ICU admission and oxygen support. Blood cultures were negative; the exhaustive infectious work up was unrevealing. In view of persistent unexplained fever and new‐onset severe thrombocytopenia, a bone marrow examination was performed and confirmed relapse of myeloma.
Laboratory investigations on presentation
| Test | Result | Reference range |
|---|---|---|
| Hemoglobin (Hb) | 7.5 g/dL | 12–16 g/dL |
| Serum calcium | 8.3 mg/dL | 8.5–10.5 mg/dL |
| Uremia | 43 mg/dL | 15–45 mg/dL |
| Serum creatinine | 1.59 mg/dL | 0.6–1.1 mg/dL |
| Estimated GFR (CKD-EPI) | 48 mL/min/1.73 m² | >90 mL/min/1.73 m² |
| Serum protein electrophoresis (SPEP) | Two monoclonal bands (beta-2 and gamma re-gions), combined 1.26g/dL | N/A |
| Serum protein electrophoresis (SPEP) after BME treatment (be-tamercaptoetha-nol) | polymerized IgA dissociates into monomers mi-grating as one sharp band (M protein -0.66 g/dL) | N/A |
| Immunotyping (IT | Broad polymeric band in IgA frac-tion; single lambda light chain band | N/A |
| β-mercaptoethanol reduction | Collapse to single IgA lambda peak | N/A |
| Serum Immuno-globulins | IgG – 657.11 mg/dL, IgM – 29.54 mg/dL, IgA – 1056.27 mg/dL | IgG –700 - 1600 mg/dL, IgM – 40 - 230 mg/dL, IgA – 70 – 400 mg/dL |
| Serum-free light chains (FLC) | Kappa: 18.4 mg/L, Lambda: 6188 mg/L, κ/λ ratio: 0.002 | Kappa: 2.3–20.73 mg/L Lambda: 4.23–27.69 mg/L, Ra-tio: 0.26–1.65 |
On SPEP with capillary electrophoresis, two separate monoclonal bands were identified: one migrating in the β2 region and the second in the γ region. This pattern is often interpreted as biclonal gammopathy. However, given the known IgA isotype (which can polymerize) and the unusual migration, further investigation was undertaken.
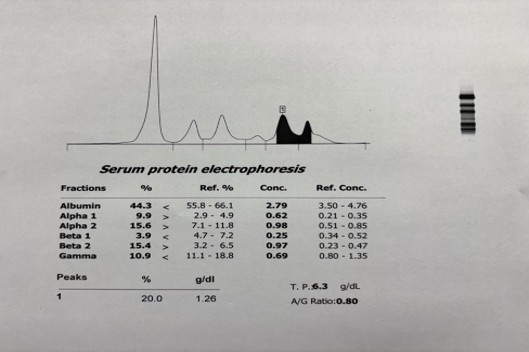
Fig(1): Serum protein capillary electrophoresis pattern.
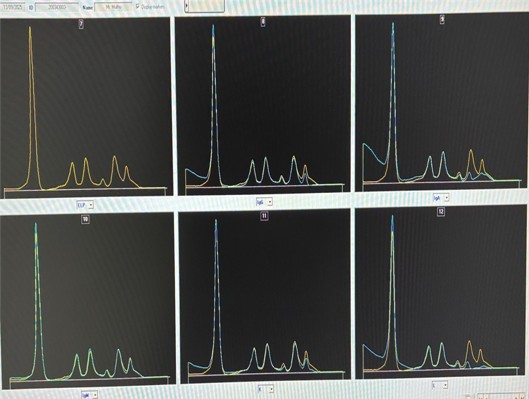
Fig(2): Serum immunosubtraction pattern(MINICAP -SEBIA).
Intervention for diagnostic clarification
Serum was treated with β mercaptoethanol (BME) as follows: Solution A (90 µL distilled water + 10 µL 1% BME); Solution B (10 µL Solution A + 90 µL Fluidil); 300 µL patient serum incubated with Solution B for 15 minutes at room temperature. After BME reduction, repeat serum electrophoresis & immunofixation revealed collapse of the two separate bands into a single sharp IgA λ peak migrating in the β2 region. This confirmed that the initial dual band appearance was due to polymeric IgA rather than true biclonality
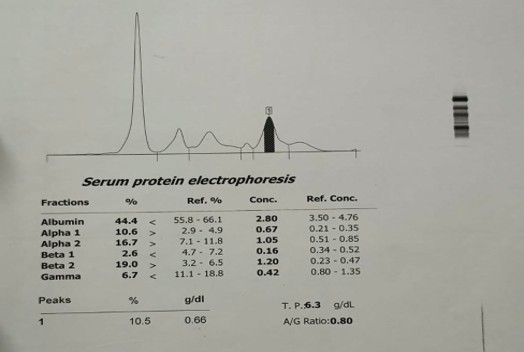
Fig(3): Serum protein capillary electrophoresis pattern after BME (betamercaptoethanol) treatment.
After BME reduction, repeat serum protein electrophoresis revealed collapse of the two separate bands into a single sharp IgA λ peak migrating in the β2 region. This confirmed that the initial dual band appearance was due to polymeric IgA rather than true biclonality
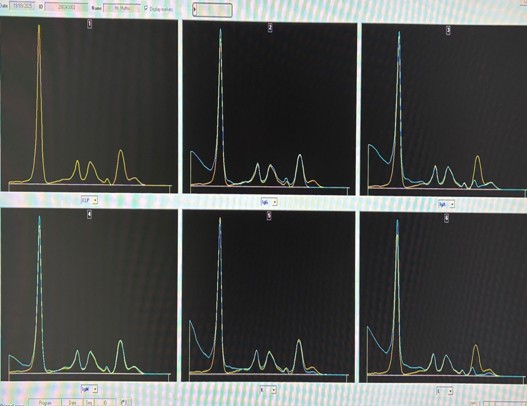
Fig (4): Serum immunosubtraction pattern after chemical treatment of the serum with BME (MINICAP -SEBIA)
After BME treatment, polymerized IgA dissociates into monomers migrating as one sharp band [5]. The patient was counselled about relapses and planned for salvage therapy with daratumumab + carfilzomib regimen. Nephroprotective strategies were initiated given impaired renal function, and close hematological monitoring instituted.
Discussion
The case illustrates key diagnostic and clinical issues:
- IgA polymerization and abnormal migration: IgA molecules can exist as monomers, dimers or higher order multimers via disulfide bonds and J chain formation; polymeric forms may migrate differently on electrophoresis, sometimes in the beta region rather than the typical gamma region. This can lead to multiple bands from the same monoclonal protein. Without awareness, this may be misinterpreted as biclonal gammopathy[2].
- Biclonal vs polymeric artefact: True biclonal gammopathy involves two distinct M proteins (often of different isotypes or light‐chain types) secreted by separate clones. In contrast, polymeric artefact arises when a single clone’s immunoglobulin forms multiple migrating species. In this case, a single λ light chain restriction plus collapse to a single peak after reduction confirms the latter[3].
- Diagnosis via reduction with BME: The use of β mercaptoethanol (BME) to reduce disulfide bonds is a simple and cost-effective tool. After BME treatment, polymerized IgA dissociates into monomers migrating as one sharp band. These aids correct interpretation of SPEP/IT and prevents overestimation of disease burden or misdiagnosis of biclonality [5].
- Clinical relevance: Accurate identification of clonality is critical in myeloma management — misclassifying polymeric IgA as two separate clones could lead to erroneous conclusions about disease complexity, prognosis or therapy. Moreover, monitoring M protein levels relies on accurate quantitation; polymeric bands could inflate measured levels and mislead response assessment [4,6].
- Implications for monitoring and complications: IgA polymerization may correlate with clinical issues such as hyper viscosity, and laboratory interferences (e.g., altered calcium measurement). For relapse monitoring, awareness of isotype specific behavior is crucial[6].
- Literature context: Previous reports note that IgA (and less commonly IgM) may migrate into the beta region or present with multiple peaks due to polymerization. Incorporation of reduction steps or advanced immunofixation techniques helps improve resolution. [2,3]
Conclusion
In patients with known or suspected IgA monoclonal gammopathy, the appearance of two monoclonal bands on SPEP should prompt consideration of IgA polymerization rather than automatic assumption of biclonal gammopathy. Chemical reduction with β mercaptoethanol is a useful adjunct to distinguish true biclonality from polymeric artefact [5]. Accurate interpretation ensures correct disease assessment, avoids overestimation of M protein burden, and guides appropriate management in plasma cell disorders.
References
- Kyle RA, Rajkumar SV. Monoclonal gammopathies of undetermined significance and smoldering multiple myeloma. Curr Hematol Malig Rep. 2010;5(2):62–69.
- Keren DF. Protein Electrophoresis in Clinical Diagnosis. 3rd ed. Chicago: ASCP Press; 2010.
- Bossuyt X. Advances in serum protein electrophoresis. Adv Clin Chem. 2006;42:43–80
- Murray DL, Puig N, Kristinsson SY, et al. Clinical utility of electrophoresis and immunofixation. Clin Biochem. 2019;64:1–10.
- Ladenson JH. Disulfide bond reduction and immunoglobulin structure in electrophoresis. Clin Chem. 1977;23(4):584–590.
- Durie BG, Harousseau JL, Miguel JS, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20(9):1467–1473.
