ASD with Partial Anomalous Pulmonary Venous Connection (PAPVC).
Pushpa1*, Anitha2, Rathika3, Bharathi4
1Operation Theater In charge, Kauvery Hospital, Heart city, Trichy, Tamil Nadu
2Operation Theater Senior Staff, Kauvery Hospital, Heart city, Trichy, Tamil Nadu
3Operation Theater Senior Staff, Kauvery Hospital, Heart city, Trichy, Tamil Nadu
4Operation Theater Secretary, Kauvery Hospital, Heart city, Trichy, Tamil Nadu
*Correspondence
Introduction
Atrial Septal Defect (ASD) is one of the most common congenital heart diseases (CHD) in children, with an estimated prevalence of roughly 1.6 per 1,000 live births (0.16%). It accounts for approximately 8% to 10% of all congenital heart defects. The prevalence is notably higher among girls. The prevalence of congenital heart disease, including ASDs, has risen over the past 50 years. Congenital heart disease was diagnosed in less than 1 per 1,000 live births in the 1930s. Recent data indicate a prevalence of 9 per 1,000 live births. Similarly, ASDs were identified in less than 0.5 per 1,000 live births between 1945 and 1949, but recent epidemiologic studies estimate their occurrence at 1.6 per 1,000 live births. This apparent increase in prevalence is likely attributed to advancements in imaging technologies and improved practitioner training rather than a true rise in disease incidence. An ASD occurs when the communication between the right and left atria fails to close. ASD encompasses defects in the true septal membrane and other abnormalities that permit communication between the atria. The 5 types of ASD, listed from most to least frequent, include patent foramen ovale, ostium secundum defect, ostium primum defect, sinus venosus defect, and coronary sinus defect. Small ASDs usually close spontaneously in childhood. Large defects that do not close on their own may require percutaneous or surgical intervention to prevent further complications, such as stroke, dysrhythmia, and pulmonary hypertension.
Patients with smaller heart defects, i.e., less than 5 mm, may not develop any symptoms. In contrast, individuals with defects ranging from 5 to 10 mm typically experience symptoms in the 4th or 5th decade of life. Patients with larger defects are present earlier, in the 3rd decade of life. Symptoms may include dyspnea, fatigue, exercise intolerance, palpitations, and signs of right-sided heart failure. Approximately 20% of adult patients develop atrial tachydysrhythmias preoperatively. Evidence of stroke or transient ischemic attack, especially following the diagnosis of a peripheral blood clot, should raise suspicion for an ASD. Atrial septum was evaluated in necropsy specimens from subjects who died under the age of one year. Observations indicated that when an atrial septal defect (ASD) was present, there was commonly an associated condition. In the vast majority, the ASD was at the fossa ovalis and took the form of valvular incompetent foramen ovale. The findings strongly support the concept that an ASD at the fossa ovalis found in symptomatic infants is acquired secondary to the effects of an underlying anomaly. Overloading of the left or right atrium appears to be the mechanism resulting in the formation of an acquired ASD.
Case Presentation
8 years aged boy had vomiting following outside food intake for which boy was taken to an outside hospital. He was diagnosed with Acyanotic congenital heart disease – ASD with Partial Anomalous Pulmonary Venous Connection (PAPVC). In view of the above findings, the patient was advised ASD surgical closure with rerouting of PAPVC.
On examination
Patient conscious, oriented
| Temp | 96.1 F |
| PR | 80 b/min |
| RR | 20 b/min |
| CVS | S1S2+ |
| Respiratory Sound | Clear |
| P/A | Soft |
| Preop Weight | 23 Kg |
| Postop Weight | 21.9 Kg, |
| BP | 90/60 mmhg |
| SpO2 | 98% at RA |
| Height | 128 cm |
| Weight | 23.34 kg |
Pre OP Medications: IVF.NS 60 mL.
Pre OP Investigations
| Hb | 12.8g/dl |
| Urea | 25mg/dl |
| Creatinine | 0.9mg/dl |
| Na | 136mmol/L |
| K | 4.03mmol/l |
| Serology | Negative |
| CAG | Not done |
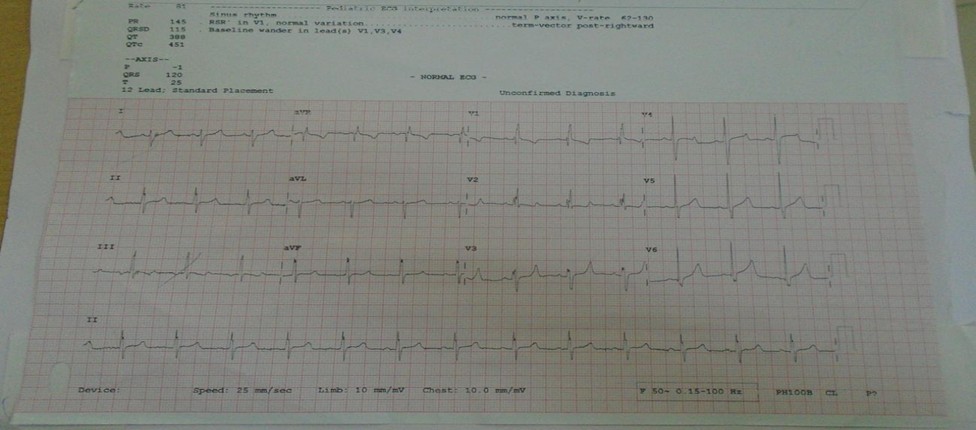
ECG
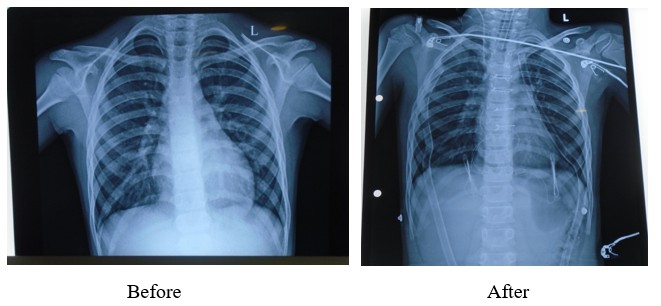
X-Ray
USG: No Significant Abnormality Detected.
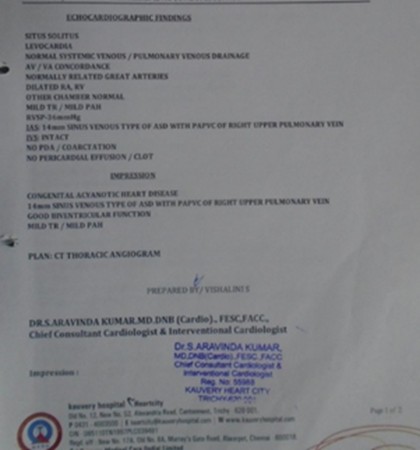
ECHO
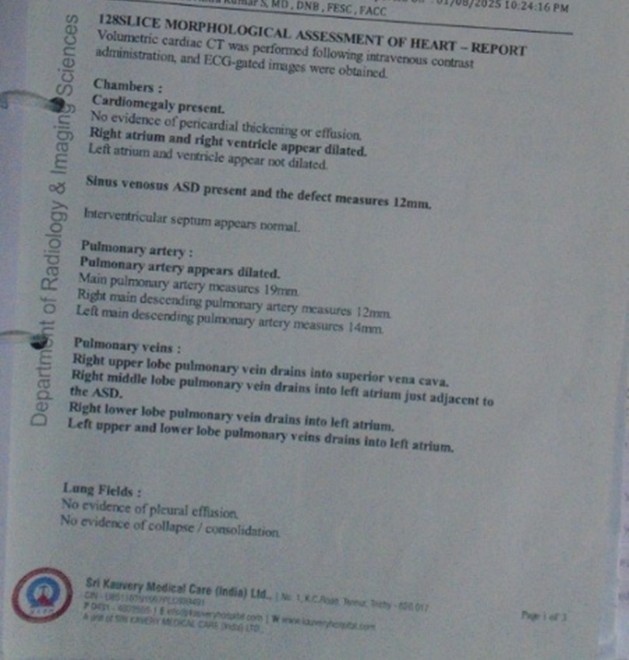
CT Scan
Impression
- Congenital Acynotic Heart Disease.
- Dilated RA&RV.
- 14MM sinus venous type of ASD with PAPVC of right upper pulmonary vein.
- Good biventricular function.
- Mild TR, mild PAH.
Operation Notes
Surgery
Closure of SVC type of ASD with rerouting of right pulmonary veins with pericardial patch/ Pericardial patch Augmentation of SVC.
Findings
- Large 6 x 3 cm SVC type of sinus venous defect seen.
- Four right side pulmonary veins seen draining into the SVC & SVC – RA junction.
- No PDA & LSVC .
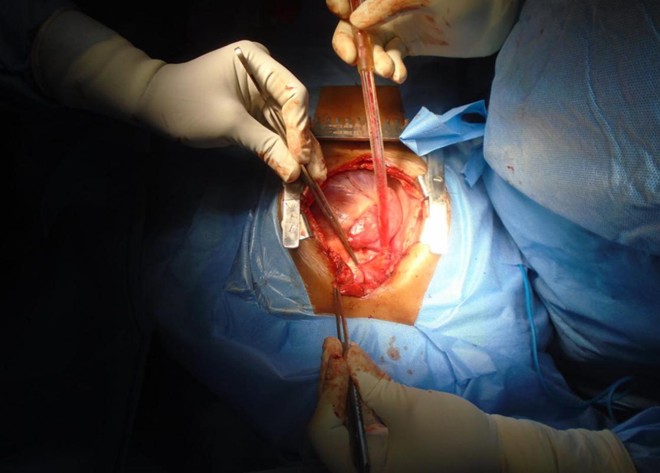
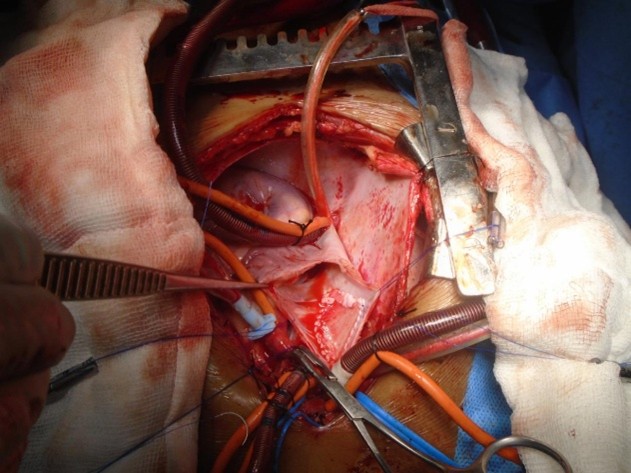
Procedure
Chest opened by a median sternotomy, pericardial patch harvested. Aortic, innominate vein/ IVC cannulation done. Antegrade DelNido plegia given. Cooled to 280C. Both cavae looped and snared. Vertical incision placed on the SVC extending across the SVC – RA junction into the RA. ASD closed with a pericardial patch rerouting the drainage of the right pulmonary veins into the LA. SVC closed with a pericardial patch using 5-0 Prolene sutures. Patient re-warmed. Weaned off CPB. Decannulation done. Sites reinforced. Patient in sinus rhythm. One atrial and one ventricular pacing wires placed. Chest closed with N6 steel wires after placing one right pleural and one mediastinal chest drains.
Procedure Images
Benefits of ASD Closure
ASD closure improves quality of life, reduces heart failure and stroke risk, and prevents long-term complications like pulmonary hypertension by allowing the heart and lungs to function normally.
Improved Heart and Lung Function: Closing the defect allows the heart to pump blood normally, preventing excess blood flow to the lungs and protecting them from damage.
Reduced Risk of Complications: Closure prevents chronic right-sided heart enlargement, pulmonary hypertension, atrial arrhythmias, and paradoxical embolism.
Post Operative Period
0 – POD
- Patient received from HCOT with AMBU bag ventilation then connected with mechanical ventilator.
- Mode – SIMV (PRVC+PS).
- Fio2 -100%, PEEP- 5cmof H2O, TV-450ml.
- Patient vitals were stable.
- He was managed with necessary support.
- Adrenaline 0.8ml/ Hr.
- NTG 0.1mL/ hr.
- Milrinone 3.5 ml.
- Dexmedetomidine 2.5ml.
- Antibiotic Inj. Supacef 75mg IV -TDS administered.
- Pan 20mg iv – OD.
- Myopyrolate 2.5 ml IV STAT.
- Fentanyl 20 mcg IV STAT.
- Para 350 mg IV STAT.
- Total ICD drain – 60ml.
- Every 4th patient was given back care and ET suctioning.
- Extubation done.
1st POD
- Patient vitals are stable.
- He managed with
- Adrenaline 0.8ml/hr.
- NTG 0.1ml/hr Stopped.
- Milrinone 3.5 ml.
- Dexmedetomidine 2ml.
- Supacef 75mg IV -TDS.
- Pan 20mg IV OD.
- Para 350 mg IV STAT.
- Ecosprin 75 mg -1/2 tablet.
- Early morning patients were given mouth-care, combing and dressing done.
- Total ICD drain -40ml.
2nd POD
- Patient vitals are stable.
- He was managed with Inj. Dexmedetomidine 2ml.
- ICD 40- ML.
- Remove Right. Radial artery/ ICD/ Pacing Wire.
- CVC removed.
- Chest Physio given.
- Nebulization given
Patient shift to ward with stable status and no complaints.
| S. No | Name of the Investigation | 0 - POD | 1st POD | 2nd POD |
|---|---|---|---|---|
| 1 | Hb | 11.1 | 9.7 | 8.2 |
| 2 | PCV | - | 26.8 | 286.8 |
| 3 | Urea | - | 34.21 | 34.21 |
| 4 | Creatinine | - | 0.37 | 0.37 |
| 5 | Na | 134 | 132 | 132 |
| 6 | K+ | 3.8 | 4.30 | 4.30 |
| 7 | Ph | 7.37 | - | - |
| 8 | PO2 | 257 | - | - |
| 9 | PCo2 | 36 | - | - |
| 10 | HCO3 | 22.8 | - | - |
| 11 | Glucose | - | - | - |
Nursing Diagnoses
- Impaired gas exchange: Related to a large left-to-right shuntthrough the ASD, leading to inadequate oxygenation and mixed blood flow.
- Activity intolerance: Secondary to fatigue and shortness of breath from the increased workload on the right side of the heart and lungs.
- Risk forpulmonary infection/recurrent respiratory infections: Due to increased blood flow to the lungs, making the child more susceptible to respiratory infections and pneumonia.
- Imbalanced nutrition: Less than body requirements– Because the child may tire easily, leading to difficulties maintaining adequate intake and slower growth.
- Risk forbleeding: Post-procedure (catheterization or surgery) due to potential for blood loss.
- Deficient knowledge: About the ASD, its treatment, and the importance of follow-up care to prevent complications like arrhythmias or stroke.
Nursing Considerations
- Monitor for symptoms: Observe for fatigue, shortness of breath during activity, and poor growth, as these may indicate a larger defect or increased strain.
- Encourage activity pacing: Teach the child to rest when tired and to limit strenuous activity to prevent excessive strain on the heart.
- Promote respiratory health: Advice on good hand hygiene to reduce exposure to respiratory pathogens.
- Support nutritional needs: Ensure adequate caloric intake to support growth and provide feeding assistance if needed.
- Provide pre- and post-procedure education: Explain the risks and benefits of surgical or catheter-based closure and provide clear instructions for post-operative care to prevent bleeding and infection.
- Educate the family: Discuss the condition, potential future complications (like arrhythmiasor stroke), and the importance of regular follow-ups with the pediatric cardiologist.
Nursing Management
Pre-Procedure Management
- Assessment and Preparation: Collect baseline blood work (CBC, electrolytes), explain the procedure, and ensure the patient’s consent is obtained.
- Patient Education: Use the AIDET(Acknowledge, Introduce, Duration, Explanation and Thank You) method to build trust and explain the procedure to the patient and family.
- NPO Status: Advise the patient to maintain a period of nothing by mouth (NPO) before the procedure.
- Aseptic Technique: Insert intravenous (IV) lines and prepare the skin using strict aseptic techniques to prevent infection.
Preoperative Management
- Surgical Instrument Management:Ensure that surgical instruments, especially occluding devices, are handled with aseptic techniques to prevent infection.
- Aseptic Technique:Enforce strict aseptic techniques to avoid introducing infection during the procedure.
- Patient Warmth:Keep the patient warm during the procedure to prevent hypothermia.
Post-Procedure & Long-Term Management
Monitoring: Continuously monitor the patient’s vital signs and hemodynamic status for any signs of complications.
Medication Administration
- Beta-blockers:To control heart rate.
- Anticoagulants:To reduce the risk of blood clots.
- Diuretics:To reduce fluid buildup.
Lifestyle Adjustments
- Diet:Advise patients to limit alcohol, sodium, and sugar intake.
- Exercise:Encourage regular, moderate exercise (E.g., 30 minutes most days of the week) to increase aerobic capacity.
- Activity Level:Gradually return to normal activities, with the possibility of a ~6-week recovery period for surgical recovery.
- Symptom Management:Reduce exercise tolerance and treat symptoms that arise from the atrial septal defect.
Nursing Roles and Collaboration
- Holistic Care:Provide care that considers both the physical and psychological needs of the patient and their family.
- Interprofessional Team:Work closely with physicians and other healthcare professionals to provide comprehensive and high-level care.
- Family Education:Educate the family on the condition, treatment, and ongoing care requirements to ensure their active participation.
Assessment and Monitoring
- Monitor Vital Signs and Oxygen Saturation: Routinely check the child’s heart rate, respiratory rate, and oxygen saturation to detect signs of worsening heart or lung function.
- Observe for Symptoms: Look for increased fatigability, breathlessness, recurrent chest infections, and growth failure, which can indicate a significant ASD burden on the heart.
- Monitor Fluid Balance: Weigh the child daily and maintain intake/output charts to manage fluid balance effectively.
- Auscultator Heart and Lung Sounds: Listen to a systolic murmur, a split S2, and any signs of fluid in the lungs.
Care Post-Procedure (Catheterization or Surgery)
- Maintain Wound Care: Keep surgical or catheterization sites clean and dry to prevent infection.
- Pain Management: Administer prescribed medications for pain and monitored the child’s comfort level.
- Activity Restrictions: Enforce activity limitations as advised by the cardiologist. Typically, quiet activities like reading, watching TV, and resting are encouraged for several weeks after surgery.
- Monitor for Complications: Be vigilant for signs of infection, bleeding, or other issues at the procedure site.
Health Education and Promotion
- Educate the Family: Provide clear instructions on ASD, self-care, and medication adherence and signs of postoperative complications.
- Promote Healthy Lifestyle: Advice on healthy dietary habits, limit sodium and sugar intake, and encourage adequate hydration.
- Exercise Guidance: Provide guidance on appropriate levels of exercise and activity, emphasizing the need for regular follow-ups with the cardiologist.
- Prevent Infection: Educate the family on good dental care and hygiene practices to reduce the risk of infection.
Medication Management
- Administer Prescribed Medications: Give medications such as diuretics(e.g., Furosemide), digoxin, and antibiotics as prescribed.
- Ensure Adherence: Emphasize the importance of taking all medications as scheduled for the prescribed duration.
- Promoting Normal Development
Encourage Quiet Activities: Support the child in engaging in quiet, enjoyable activities at home and promote relaxation and recovery.
- Facilitate Return to School: Follow the cardiologist’s advice regarding when the child can return to school.
- Emotional Needs: Help the child and family cope with stress and fear associated with diagnosis and treatment.
Conclusion
Children with ASDs require consistent follow-up with cardiologists to monitor heart structure and function, as well as hemodynamic status. Clinicians should monitor asymptomatic patients. All affected individuals should be educated that elective closure reduces the risk of pulmonary hypertension.
The nurse should help ensure the patient has regular follow-up appointments. During follow-up after the procedure, the nurse should monitor the patient for changes in vital signs, new murmurs, or unexplained fever. Open communication between the interprofessional teams is recommended to achieve the best outcomes with minimal complications.
Reference
- Meissner I, Whisnant JP, Khandheria BK, Spittell PC, O’Fallon WM, Pascoe RD, Enriquez-Sarano M, Seward JB, Covalt JL, Sicks JD, Wiebers DO. Prevalence of potential risk factors for stroke assessed by transesophageal echocardiography and carotid ultrasonography: the SPARC study. Stroke Prevention: Assessment of Risk in a Community. Mayo Clin Proc. 1999 Sep;74(9):862-9. [PubMed]
- Celermajer DS. Atrial septal defects: even simple congenital heart diseases can be complicated. Eur Heart J. 2018 Mar 21;39(12):999-1001. [PubMed]
- Aoki H, Horie M. Electrical disorders in atrial septal defect: genetics and heritability. J Thorac Dis. 2018 Sep;10(Suppl 24):S2848-S2853. [PMC free article] [PubMed]
- Torres AJ. Hemodynamic assessment of atrial septal defects. J Thorac Dis. 2018 Sep;10(Suppl 24):S2882-S2889. [PMC free article] [PubMed]
- Chelu RG, Horowitz M, Sucha D, Kardys I, Ingremeau D, Vasanawala S, Nieman K, Paul JF, Hsiao A. Evaluation of atrial septal defects with 4D flow MRI-multilevel and inter-reader reproducibility for quantification of shunt severity. MAGMA. 2019 Apr;32(2):269-279. [PMC free article] [PubMed]
- van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, Roos-Hesselink JW. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011 Nov 15;58(21):2241-7. [PubMed]
- Kloesel B, DiNardo JA, Body SC. Cardiac Embryology and Molecular Mechanisms of Congenital Heart Disease: A Primer for Anesthesiologists. Anesth Analg. 2016 Sep;123(3):551-69. [PMC free article] [PubMed]
- Naqvi N, McCarthy KP, Ho SY. Anatomy of the atrial septum and interatrial communications. J Thorac Dis. 2018 Sep;10(Suppl 24):S2837-S2847. [PMC free article] [PubMed]
- Naik RJ, Shah NC. Teenage heart murmurs. Pediatr Clin North Am. 2014 Feb;61(1):1-16. [PubMed]
- El-Segaier M, Pesonen E, Lukkarinen S, Peters K, Ingemansson J, Sörnmo L, Sepponen R. Atrial septal defect: a diagnostic approach. Med Biol Eng Comput. 2006 Sep;44(9):739-PubMed]
