The Gateway to Quality Care: Evidence-Based Initial Patient Assessment
Divya 1*, Muthulakshmi. P2, Deepa Rani3
1Staff nurse [NRP], Kauvery Hospital, Radial Road, Chennai, Tamil Nadu
2Clinical instructor, Kauvery Hospital, Radial Road, Chennai, Tamil Nadu
3Deputy Nursing Superintendent, Kauvery Hospital, Radial Road, Chennai, Tamil Nadu
*Correspondence
Introduction
The initial assessment is the foundation of quality nursing care. It is the first step a nurse takes when a patient is admitted to the hospital. It helps the nurse understand the patient’s current health condition, need and problem. This assessment gives a complete picture of the patient’s physical, mental and emotional status. It also helps to plan proper nursing care and treatment.
![]()
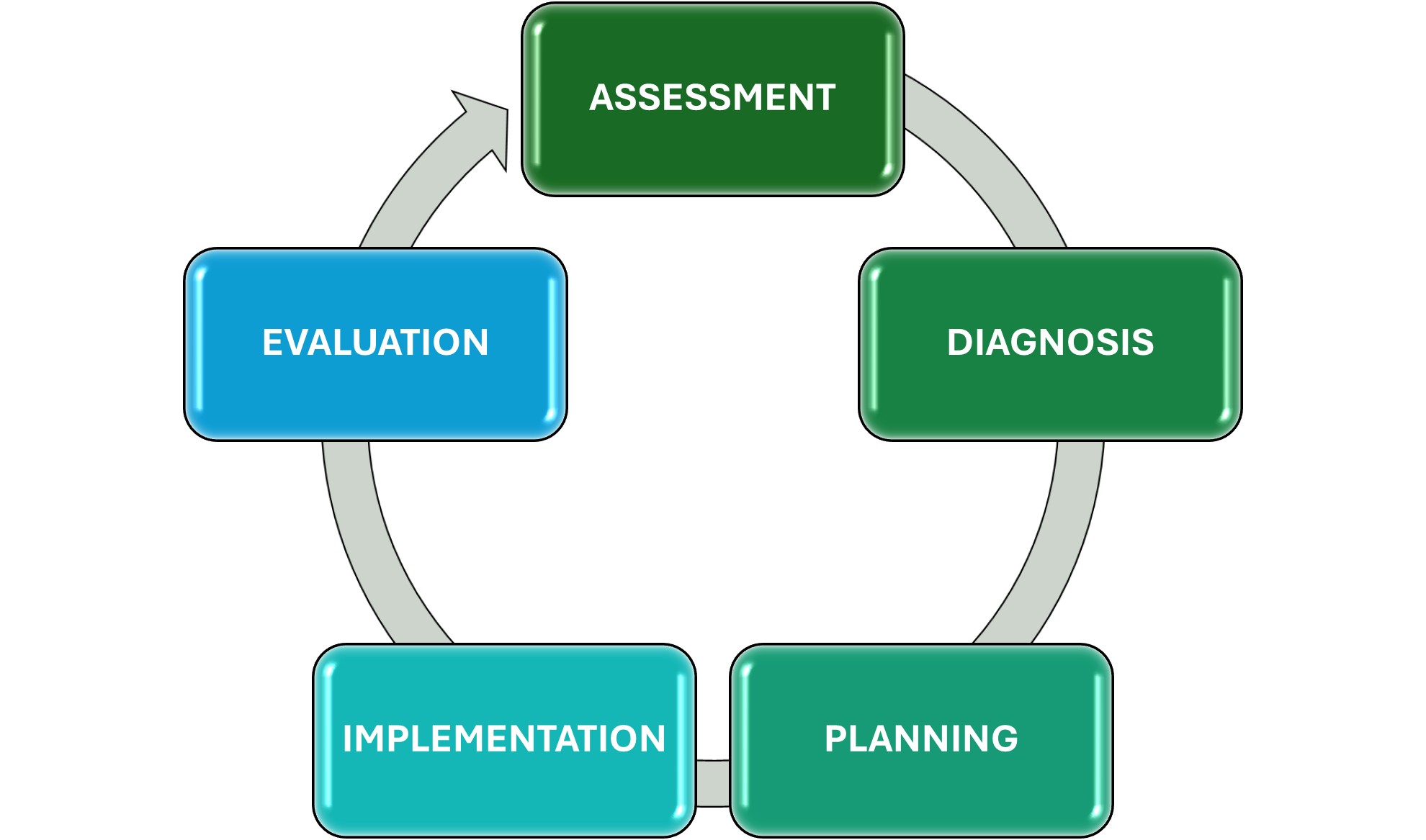
Assessment: The registered nurse collects comprehensive data pertinent to the patient’s health or situation.
Diagnosis: The registered nurse analyzes the assessment data to determine the diagnosis or issues.
Planning: The registered nurse develops a plan that prescribes strategies and alternatives to attain expected outcomes.
Implementation: The registered nurse implements the identified plan.
Evaluation: The registered nurse evaluates progress to the ward attainment of outcomes.
TRIAGE
Triage is the initial, rapid assessment in a hospital to prioritize patients based on the severity of their condition for treatment. It involves a trained nurse or medical professional quickly evaluating a patient’s vital signs, performing a visual and brief focused physical assessment, and collecting a short history to determine if they need immediate, urgent or less urgent care.
Triage system
| Red | Immediate care |
| Yellow | Urgent care |
| Green | Less urgent care |
| Black | Not able to survive |
Red: Patients require immediate treatment.
Yellow: Patients are stable at the moment and there is not any immediate danger but it will require observation.
Green: Patients who require medical treatment at some point, once more critical injuries have been treated.
Black: For those who are already deceased or for patients whose injuries are so extensive that they will not be able to survive, given the level of care available.
Initial assessment
Definition
Initial assessment is the first and most complete evaluation of a patient’s health status done by a nurse or doctor immediately after the patient’s admission or arrival to the hospital.
It is the comprehensive evaluation done for a patient [Out-patient, Day-care, In-patient and Emergency] when they first enter the hospital or healthcare facility.
Assessment based on
- Time and mode of arrival.
- Based on triage system.
- Chief complaints / Major observations.
- Vitals sign / Allergy history.
- Past medical history with duration.
- Surgical history with duration.
- Functional assessment.
- Level of consciousness.
- Vulnerability assessment.
- Pain assessment.
- Fall risk assessment.
- DVT assessment.
- Pressure injury assessment.
- Head to toe assessment.
- Medical assessment.
- Diagnostic imaging procedures.
- Laboratory investigations.
- Therapeutic procedures.
- Monitoring and supportive care.
- Preventive and Rehabilitation care.
- Handed over valuables to patient or Patient attender and family education.
- Nursing care plan.
Time and Mode of arrival
The process of assessing a patient’s condition is based on when they arrive and how they arrive to determine the urgency and priority of care.
Time of arrival: Guided urgency of assessment
Mode of arrival
Guides prioritize patient condition.
- Ambulance
- Stretcher
- Walking
- With assistance
- Wheelchair
Based on triage system
Triage assessment is the process of prioritizing patients on arrival at the hospital based on the severity of their condition, urgency of care needed and risk to life, to ensure timely and appropriate treatment.
- Red – Immediate care
- Yellow – Urgent care
- Green – Non – urgent care
- Black – Expectant [Palliative comfort care]
Chief complaints
Chief complaint is the primary reason for which a patient seeks medical care, expressed in the patient’s own words. It guides the nurse and doctor in planning assessment and treatment.
Example: “Fever and cough for 3days”, “Severe abdominal pain since last night”.
Major observations
Major observations are the critical signs and parameter monitored by nurses during the initial and ongoing assessment to evaluate a patient’s health status and detect any changes or complications.
Example: Vital signs, LOC, Pain assessment, Physical observations, Fluid, Nutrition status, Safety, Risk factors, Psychological and Emotional status.
Vital sign
Vital signs are important indicators of health states of the body [or] Signs of life especially pulse, respiration, body, temperature, blood pressure and pain.
Vital parameters
| Height | Body length |
|---|---|
| Weight | Body mass |
| BMI | Weight (Kg)/ Height (cm) |
| Temperature | 37.5 C [99.5 F] |
| Pulse | 60-100 beats/min |
| Heart rate | 60-100 beats/min |
| Respiration | 12-20 breaths/rate |
| Blood pressure | 120/80mmhg. [Systolic: 90-120mmhg\Diastolic: 60-80mmhg] |
| SPO2 | 95-100% |
| CBG | F (70-100mg/dl), PP (<140mg/dl), Random [70-140mg/dl] |
| Pain score | [0-10 in scale] |
| GCS | E4+V5+M6 = GCS [15] |
AVPU in emergency care
Allergy history
Allergy history is the systemic collection of information about a patient’s past or current allergic reactions to drugs, foods, blood, environmental factors or other substances. It helps prevent adverse reactions and ensures safe care.
| Allergen name | |
| Type of reaction | |
| Severity | |
| Date | |
| Onset of reaction | |
| Treatment given based on allergic reaction | |
| Details of documented |
Past medical history
Past medical history with duration is a detailed record of previous health conditions along with how long the patient has had them. It helps nurses and doctors provide safe, personalized care.
Surgical history
Surgical history with duration is a record of all part surgeries a patient has undergone, including the type of surgery, date or year and duration since surgery. This helps in planning current care and identifying any complications or precautions.
Functional assessment
The process of evaluating a patient’s ability to perform daily activities and essential life tasks independently, including physical, psychological and social functioning. It helps nurses plan care, identify limitations and promote patient independence.
Level of consciousness
The States of a patient’s awareness and responsiveness to the environment, including alertness, orientation and ability to respond to stimuli. It is a critical observation in nursing assessment to detect neurological or systemic problems.
Parameters: Alertness, confusion, lethargy, obtunded, stupor, coma.
Tools: Glasgow coma scale [GCS], Alert [AVPU Scale], Verbal response, Pain response, Unresponsive.
Vulnerability assessment
- Vulnerability assessment helps nurses find patients who need extra care and protection to keep them safe from harm or neglect.
- Elderly patients, children, pregnant women, mentally ill (or) unconscious patients, physically disabled (or) bedridden patients.
Pain assessment
- Pain assessment is the process of identifying, measuring and evaluating a patient’s pain level-including its location, intensity, type, duration, and factors affecting it-to plan effective pain management and comfort care.
- Numeric rating scale, Visual analogue scale, Wong-baker faces scale, (PQRST) Method.
Fall risk assessment
Identify patients likely to fall and take preventive actions to ensure safety and avoid injury as per NABH (National Accreditation Board for Hospitals) patient safety standards. (Fall risk assessment chart).
DVT assessment
Identify patients at risk of blood clots in deep veins, so they can prevent complications and ensure patient safety as per NABH (National Accreditation Board for Hospitals) Standards. (DVT Assessment Chart).
Pressure injury assessment
Identify patients early skin damage from pressure and take steps to prevent sores and promote healing as required by NABH (National Accreditation Board for Hospitals) patient safety standards.
Head-to-toe assessment
A systematic and complete physical examination of a patient from the head down to the feet to identify any abnormalities, monitor health status and plan nursing care.
Steps of Head-to-Toe assessment
- General Appearance.
- Head and face.
- Neck
- Chest and Lungs (Respiratory system).
- Cardiovascular system.
- Abdomen (Gastrointestinal system).
- Genitourinary system.
- Musculoskeletal system.
- Skin (Integumentary system).
- Neurological system.
Medical Assessment
A medical assessment in nursing is part of the nursing assessment where the nurse collects and records information about the patient’s medical condition, including the diagnosis, medical history, treatment and ongoing management.
Components of medical assessment:
- Present Medical Condition.
- Past Medical History.
- Surgical History.
- Medication History.
- Family Medical History.
- Diagnostic and Laboratory Findings.
- Treatment and Management Plan.
- Prognosis and follow up.
Diagnostic imaging procedures
- Diagnostic imaging procedures are tests that as different types of energy (like x-rays, sound waves, magnetic fields, or radioactive substances) to create pictures of the inside of the body.
- These images help doctors diagnose diseases, monitor conditions and plan of treatment.
- ECG, CT scan, MRI, ECHO, EEG, Ultrasound, X-ray, Mammography.
Laboratory Investigations
Laboratory investigations are medical tests performed on blood, Urine, Stool or other body fluids to help diagnose, monitor, and evaluate a patient’s health condition.
- CBC, FBS, RBS, PPBS, Blood Urea & Serum Creatinine, Liver Function Test (LFT), Lipid Profile, Electrolytes (Na +k +, cl) Serology (HIV, HBsAg, VDRL), Coagulation Profile (PT, INR) Blood Grouping & Cross – Matching.
- Routine Urine Culture & Sensitivity, Pregnancy Test (Urine HCG), 24 Hour Urine Routine.
- Routine Stool Test, Occult Blood Test, Stool Culture.
Therapeutic Procedures
Therapeutic procedures are medical or nursing interventions performed to treat a disease, promote healing or improve a patient’s physical and mental well-being.
Common types of therapeutic procedures
- Oxygen therapy.
- Intravenous therapy.
- Blood transfusion.
- Wound care / Dressing.
- Nebulization
- Catheterization.
- Enema.
- Suctioning.
- Physiotherapy/Range of motion exercises.
- Nutritional therapy.
Monitoring and supportive care
Monitoring and supportive care mean the continuous observation and maintenance of a patient’s vital function to ensure stability, detect changes early and support recovery.
Components of Monitoring
Vital signs, Intake and output, Level of consciousness, Pain Assessment, Cardiac and Respiratory Monitoring, Lab and Diagnostic Reports.
Supportive Care Includes
Oxygen therapy, IV fluids and Nutrition positioning and Hygiene, Pain and Comfort measures, Emotional support, Medication administration.
Preventive and Rehabilitation Care
- Preventive care: Aims to stop diseases before they occur or worsen.
Types:
Primary prevention, Secondary Prevention, Tertiary Prevention.
- Rehabilitation care
- Patients restore normal life and function after illness, surgery or injury.
- It focuses on physical, mental, and social recovery.
- Preventive and Rehabilitation care help in reducing disease burden, improving recovery and enhancing the patient’s quality of life.
Handing over valuables to patient or patient attender
Returning the patient’s personal belongings or valuable items safely to the patient or their attender with proper documentation and acknowledgement.
Family education
Family education ensures continuity of care, patient safety and better recovery outcomes, while fulfilling NABH Standards (National Accreditation Board for Hospitals) for patient-centered and quality healthcare.
Nursing care plan
A Nursing care plan is a written guide prepared by nurses during the initial assessment to identify the patient’s health problems, set goals and plan nursing actions to achieve the best possible outcomes.
- Assessment, Diagnosis, Planning, Implementation, Evaluation.
Record
- A record is a permanent written communication that documents information relevant to a client’s health care management.
- A record is a clinical, scientific, administrative and legal document relating to the nursing care given to the individual family or community.
Report
Reports are oral or written exchanges of information shared between care givers or workers in number of ways. The report is a summary of the services of people or personnel and of the agency.
Summary
The initial nursing assessment is a comprehensive and systematic evaluation of a patient’s physical, psychological, social and medical status at the time of admission. The critical process establishes the foundation for individualized nursing care planning. By identifying actual and potential health concerns early, it ensures patient safety, enhances care coordination, and supports the delivery of high-quality healthcare in alignment with NABH standards.
Conclusion
The initial assessment serves as the cornerstone of holistic nursing practice. Through timely identification of patient needs and risks, it facilitates prompt interventions, promotes recovery, and minimizes the likelihood of complications. Furthermore, a structured and thorough assessment process reinforces the NABH commitment to patient-centered, safe, and quality-driven healthcare delivery.
