A rare case of multiple large bowel perforations following air blast injury through the rectum
Subin*
Nursing Supervisor, Department of critical care, Kauvery Hospital, Hosur, Tamil Nadu
*Correspondence
Abstract
Air blast injuries to the rectum are rare but potentially life-threatening conditions that can result in severe colorectal damage and peritonitis. These injuries often occur due to accidental or intentional insertion of compressed air into the rectum, leading to rapid colonic distension and perforation. We report a case of a 40-year-old male who presented with severe abdominal pain following an air compressor injury through the rectum at his workplace. Imaging revealed multiple large bowel perforations requiring emergency surgical intervention. The patient underwent emergency laparotomy with left colon resection and end colostomy. Postoperatively, the patient developed intestinal obstruction due to internal herniation, requiring re-exploration surgery. With timely surgical management, appropriate postoperative care, and nursing support, the patient recovered well and was discharged in stable condition. This case highlights the importance of early diagnosis and prompt surgical management in traumatic bowel perforation.
Key words: Air blast injuries; Traumatic colorectal perforation; Peritoneal cavity.
Introduction
Traumatic colorectal perforation due to compressed air injury is a rare but serious surgical emergency. The colon, particularly the sigmoid colon, is highly susceptible to injury due to its relatively fixed position and anatomical structure. Sudden high-pressure air entering through the rectum can cause rapid distension of the bowel, leading to perforation and faecal contamination of the peritoneal cavity. Such injuries are most reported in industrial settings where compressed air equipment is used. Delayed diagnosis may lead to severe complications including peritonitis, sepsis, and intestinal obstruction. Early surgical intervention is essential to prevent morbidity and mortality.
This report describes a case of traumatic multiple large bowel perforation following an air blast injury through the rectum and highlights the importance of prompt diagnosis, surgical management, and postoperative care.
Presenting Complaints
A 40-year-old male was brought to the emergency department with an alleged history of air blast injury per rectum. According to the history provided, his friend inserted an air compressor pipe into the anal region.
The patient developed:
- Severe abdominal pain.
- History of abdominal injury.
There was no history of vomiting, seizures, ENT bleeding, or loss of consciousness. The patient initially received treatment at an outside hospital and was subsequently referred to our hospital for further evaluation and management.
Past History: No significant past medical history.
Past Surgical History: Nil.
Clinical Examination
Conscious and oriented.
| Temperature | 98°F |
| BP | 100/60 mmHg |
| PR | 88 beats per minute |
| RR | 22 breaths per minute |
| SPO2 | 97% on RA |
Investigations
| Investigations | Pre Op | Post Op |
|---|---|---|
| Hb | 13.8 g/dl | 13.8 g/dl |
| PCV | 41.3 % | 41.5 % |
| Platelet | 147000 Cells/ mm3 | 332000 Cells/mm3 |
| WBC | 12820 Cells/ mm3 | 15710 Cells/ mm3 |
| Urea | 19.2 mg/dl | - |
| Creatinine | 0.8 mg/dl | - |
| Sodium | 136 mmol/L | 138 mmol/L |
| Potassium | 3.8 mmol/L | 3.8 mmol/L |
| Serology | Negative | - |
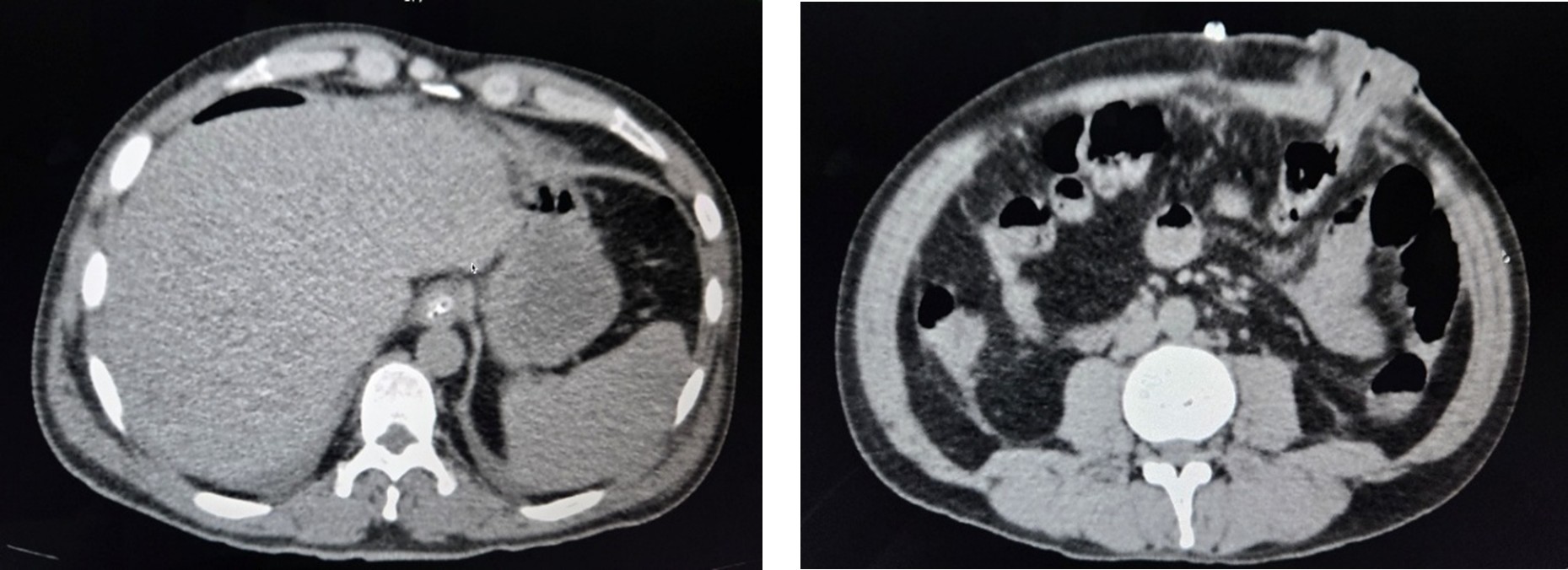
CT Report
CT abdomen revealed colon perforation with intestinal obstruction, requiring emergency surgical management.
Pre Operative
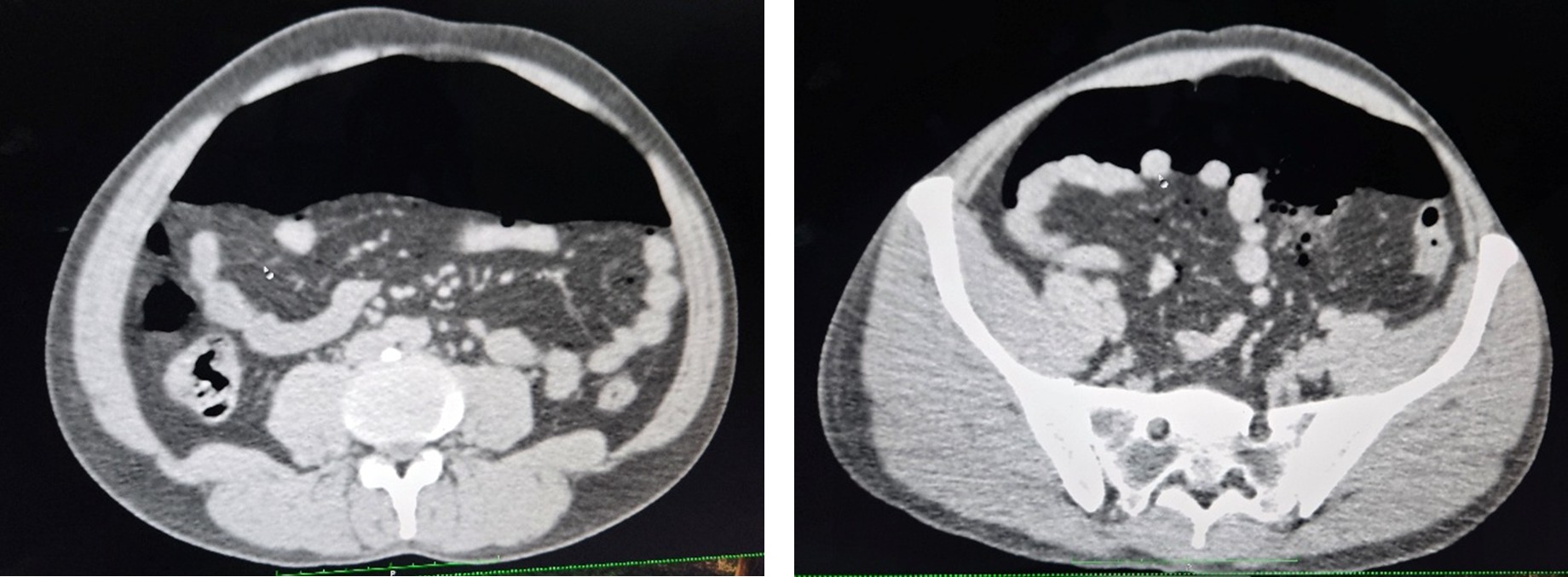
Post Operative
Clinical Presentation
The intraoperative period during the initial surgery was uneventful. Following the procedure, the patient was shifted to the Intensive Care Unit for close monitoring. Postoperatively, the patient was managed with intravenous fluids, broad-spectrum antibiotics, epidural analgesics, antiemetics, analgesics, and parenteral nutrition. Supportive respiratory care including chest physiotherapy, nebulisation, and incentive spirometry was also provided.
On Postoperative Day 1, the patient remained hemodynamically stable. The Ryle’s tube was removed, and oral feeds were initiated gradually.
On Postoperative Day 2, the patient developed abdominal distension and experienced two episodes of bilious vomiting. The Ryle’s tube was reinserted for gastric decompression, and the patient was kept under close observation. Serum electrolytes were monitored regularly and corrected as required.
On Postoperative Day 3, the patient continued to have abdominal distension with increased Ryle’s tube output. A CT abdomen was performed, which showed postoperative changes without definite evidence of obstruction.
On Postoperative Day 4, the abdominal drain was removed after assessing minimal output and stable clinical condition.
On Postoperative Day 5, the patient developed significantly increased Ryle’s tube output (approximately 1713 ml) along with a non-functioning stoma. A CT abdomen with oral contrast was performed, which revealed dilated proximal jejunal loops with absence of contrast flow beyond the fourth part of the duodenum, suggestive of intestinal obstruction.
After explaining the patient’s clinical condition to the attendants and obtaining informed consent, the patient underwent re-exploration surgery. Intraoperatively, internal herniation of proximal jejunal loops between the edge of the transverse mesocolon and the abdominal wall was identified along with inter-bowel inflammatory adhesions. The herniated loops were reduced, and stoma repositioning was performed.
Following the second surgery, the patient showed gradual clinical improvement. The Foley’s catheter was removed on Postoperative Day 6, and the patient was able to tolerate oral diet well with a functioning stoma.
The patient continued to recover without further complications and was discharged in stable condition with advice for stoma care, dietary modifications, and follow-up.
Postoperative Management
Postoperative care focused on stabilizing the patient, preventing complications, and promoting recovery following surgical intervention.
- Continuous monitoring of vital signs including blood pressure, pulse rate, respiratory rate, temperature, and oxygen saturation.
- Pain management using prescribed analgesics and epidural analgesia when required.
- Fluid and electrolyte management through intravenous fluids and regular electrolyte monitoring.
- Administration of broad-spectrum antibiotics to prevent postoperative infection.
- Provision of nutritional support, including parenteral nutrition initially, followed by gradual introduction of oral feeds as tolerated.
- Colostomy care and monitoring to ensure proper stoma function and prevent complications.
- Chest physiotherapy, nebulisation, and incentive spirometry to prevent postoperative respiratory complications.
- Continuous postoperative monitoring to detect early signs of complications such as infection, intestinal obstruction, or sepsis.
Nursing Management
Nursing care played an essential role in the patient’s postoperative recovery by ensuring close monitoring, effective wound care, and patient education.
Monitoring and Assessment
- Regular monitoring of vital signs to assess the patient’s clinical condition.
- Assessment of abdominal pain, abdominal distension, and bowel activity.
- Monitored Ryle’s tube output for gastric decompression and early identification of complications.
- Maintained an accurate intake and output chart to monitor fluid balance.
- Observed postoperative complications such as infection, intestinal obstruction, or stoma dysfunction.
Wound and Stoma Care
- Assessed the dressing of the surgical wound to prevent infection.
- Monitoring the colostomy site and stoma function.
- Ensured proper colostomy bag care and hygiene.
- Observed the stoma for complications such as oedema, bleeding, or skin irritation.
Medication Administration
- Administered the prescribed medications including antibiotics, analgesics, antiemetics, and other supportive drugs.
- Monitored the patient for therapeutic response and possible adverse reactions.
Patient Education
- Educated to the patient and family members regarding colostomy care and hygiene.
- Provided on dietary modifications and stoma care after discharge.
- Informed the patient about warning signs of complications that require medical attention.
Outcome
The patient underwent emergency laparotomy with left colon resection and end colostomy for management of traumatic multiple large bowel perforations caused by compressed air injury. During the postoperative period, the patient developed intestinal obstruction secondary to internal herniation, which required re-exploration surgery and stoma repositioning.
Following the second surgical intervention, the patient showed gradual clinical improvement with stabilization of vital signs, resolution of abdominal distension, and restoration of bowel function. The stoma began functioning adequately, and the patient tolerated oral feeding without further complications.
With appropriate surgical management, postoperative care, and nursing support, the patient recovered satisfactorily and was discharged in stable condition with advice for stoma care, dietary modification, and follow-up.
Discharge Advice
General Advice
- Maintain proper colostomy care and hygiene.
- Observe the stoma site regularly for redness, swelling, bleeding, or discharge.
- Maintain adequate hydration and balanced nutrition.
- Avoid heavy lifting or strenuous activities during the recovery period.
- Attend regular follow-up visits as advised by the surgeon.
Dietary Advice
- Follow a high-protein diet to promote wound healing and recovery.
- Consume easily digestible foods initially and gradually return to a normal diet.
- Avoid foods that may cause excessive gas, abdominal discomfort, or stoma blockage.
Warning Signs
- Severe abdominal pain.
- Fever or signs of infection.
- Persistent vomiting.
- Stoma discoloration, bleeding, or non-functioning stoma.
- Excessive abdominal distension.
Discussion – Medical Aspects
Compressed air injuries to the rectum are rare but potentially life-threatening conditions that can result in significant colorectal trauma. High-pressure air entering through the anal canal causes rapid distension of the colon, which may exceed the bowel wall’s tensile strength and lead to multiple perforations. The sigmoid colon and rectosigmoid junction are commonly affected because of their anatomical configuration and relatively fixed position.
These injuries are most frequently reported in industrial or workplace environments where compressed air equipment is used. The sudden increase in intraluminal pressure may lead to bowel perforation, faecal contamination, hemoperitoneum, and peritonitis. If not diagnosed and treated promptly, complications such as sepsis, septic shock, and intestinal obstruction may occur.
Early diagnosis relies on clinical assessment and radiological imaging, particularly CT abdomen, which helps identify bowel perforation, pneumoperitoneum, and intra-abdominal contamination. In cases of multiple bowel perforations or extensive contamination, emergency laparotomy with bowel resection and colostomy formation is often required.
In the present case, the patient sustained multiple perforations involving the sigmoid colon, descending colon, splenic flexure, and distal transverse colon, necessitating left colon resection and end colostomy. Postoperatively, the patient developed intestinal obstruction due to internal herniation, which required re-exploration surgery. Timely surgical intervention and close postoperative monitoring played a crucial role in preventing further complications and ensuring patient recovery.
Discussion – Nursing Aspects
Nursing care is an essential component in the management and recovery of patients undergoing major abdominal surgery and colostomy formation. Continuous nursing assessment helps in the early identification of postoperative complications, including infection, bowel obstruction, and stoma dysfunction.
Postoperative nursing management focuses on monitoring vital signs, assessing abdominal symptoms, and maintaining fluid and electrolyte balance. Monitoring Ryle’s tube output and maintaining an accurate intake-output chart are important to evaluate gastrointestinal function and prevent dehydration or electrolyte imbalance.
Effective wound and stoma care are also critical nursing responsibilities. Regular inspection of the surgical incision and colostomy site helps detect early signs of infection, bleeding, or stoma complications such as oedema or skin irritation. Proper colostomy bag care and skin protection around the stoma are necessary to maintain patient comfort and prevent skin breakdown.
Patient education is another important nursing role. Teaching patients and their family members about colostomy care, hygiene practices, dietary modifications, and warning signs of complications helps improve self-care and quality of life after discharge.
In this case, comprehensive nursing management, patient education, and supportive care contributed significantly to the patient’s successful recovery and adaptation to living with a colostomy.
Conclusion
Traumatic large bowel perforation due to compressed air injury per rectum is a rare but serious surgical emergency that requires immediate recognition and prompt intervention. Rapid diagnosis through clinical assessment and imaging, followed by early surgical management, is essential to prevent life-threatening complications such as peritonitis and sepsis.
This case demonstrates the importance of timely emergency laparotomy, appropriate postoperative care, and multidisciplinary management in achieving a favourable outcome. In addition, effective nursing care and patient education play a critical role in postoperative recovery and long-term adaptation to colostomy care.
Early recognition, prompt surgical treatment, and comprehensive postoperative management are key factors in reducing morbidity and improving patient outcomes in traumatic colorectal injuries caused by compressed air.
