Carcinoma of the lower esophagus managed by video-assisted thoracoscopic esophagectomy
Sahaya Saranya*, Priya
Staff Nurse, Kauvery Hospital, Hosur, Tamil Nadu
*Correspondence
Abstract
Carcinoma of the oesophagus is an aggressive malignancy with a rising global incidence. Tumours involving the lower third of the esophagus are commonly squamous cell carcinomas or adenocarcinomas, often presenting with progressive dysphagia, weight loss, and retrosternal discomfort. Early detection and timely surgical intervention significantly improve clinical outcomes. We report the case of a 67-year-old male who presented with progressive dysphagia and recurrent vomiting. Upper gastrointestinal endoscopy and biopsy confirmed squamous cell carcinoma of the lower oesophagus. Imaging revealed localized disease without distant metastasis. The patient underwent video-assisted thoracoscopic esophagectomy (VATS) with gastric pull-up reconstruction. Postoperative recovery included transient respiratory complications and febrile episodes, managed with antibiotics, supportive care, and aggressive pulmonary rehabilitation. The patient was discharged in stable condition with a feeding jejunostomy tube in-situ. This case highlights the importance of early recognition, multidisciplinary intervention, and comprehensive perioperative care in managing lower oesophageal carcinoma.
Key words: Carcinoma; Video-assisted thoracoscopic esophagectomy (VATS); Esophageal squamous cell carcinoma (ESCC)
Introduction
Esophageal squamous cell carcinoma (ESCC) is among the most prevalent types of esophageal cancer worldwide, especially in Asia. It arises from the squamous epithelium lining the esophagus and is strongly associated with chronic mucosal irritation from smoking, alcohol consumption, and habitual intake of extremely hot beverages. Patients typically present with progressive dysphagia, weight loss, regurgitation, and chest discomfort. Due to its asymptomatic early course and rapid progression, esophageal cancer is often diagnosed at an advanced stage, contributing to poor five-year survival rates ranging from 15–25%. This case illustrates the interplay between esophageal malignancy, comorbid conditions (hypertension, COPD, cerebrovascular accident), and lifestyle risk factors such as smoking.
Case Presentation
A 67-year-old male presented with progressive difficulty in swallowing and recurrent vomiting over several months. The symptoms significantly impaired oral intake and led to weight loss and generalized weakness.
Chief Complaints
- Difficulty in swallowing for 3 months.
- Multiple vomiting episodes for 2 months.
- Retrosternal discomfort while swallowing for 2 months.
- Occasional regurgitation of undigested food for 1 month.
- Loss of appetite.
History of Present Illness
The patient was asymptomatic three months prior to presentation when he developed difficulty swallowing solid foods. Dysphagia progressively worsened to include semisolids and subsequently liquids.
- Burning sensation in the chest.
- Regurgitation of food after meals.
- Unintentional weight loss of 8 kg in 2 months.
- Fatigue and generalized weakness.
- No history of hematemesis or melena was noted.
Past Medical History
- Cerebrovascular accident.
- Hypertension.
- COPD
- On regular medications in medical conditions.
- No previous surgical history.
Personal History
- Chronic smoker (25 years).
- Occasional alcohol consumption.
- Mixed diet.
- Poor oral intake in recent months.
Clinical Examination
General Examination
- Moderately built, poorly nourished.
- Pallor present.
- No peripheral lymphadenopathy.
Vital Signs
| BP | 130/70 mmHg |
| Pulse | 76 beats/min |
| Respiratory Rate | 20 breaths/min |
| SpO2 | 98% on room air |
| Temperature | 96°F |
Investigations
| Lab Test | Pre Op | Post Op |
|---|---|---|
| Hb | 8.6g/dl | 12.7g/dl |
| PCV | 26.4% | 38.7% |
| WBC | 10620 cells/mm3 | 6270 cells/mm3 |
| Platelet | 195000 cells/Cumm | 163000 cells/Cumm |
| Sodium | 130mmol/L | 134mmol/L |
| Potassium | 2.63mmol/L | 4.4mmol/L |
| PH | 7.61 | 7.33 |
| PCO2 | 30 mmHg | 49 mmHg |
| PO2 | 69mm Hg | 90mm Hg |
| HCO3 | 30.1 mmol/L | 25.8 mmol/L |
| Creatinine | 1.8mg/dl | 1.3mg/dl |
Upper Gastrointestinal Endoscopy
- Ulceroproliferative lesion in the lower esophagus.
- Partially obstructing the lumen.
- Multiple biopsies taken.
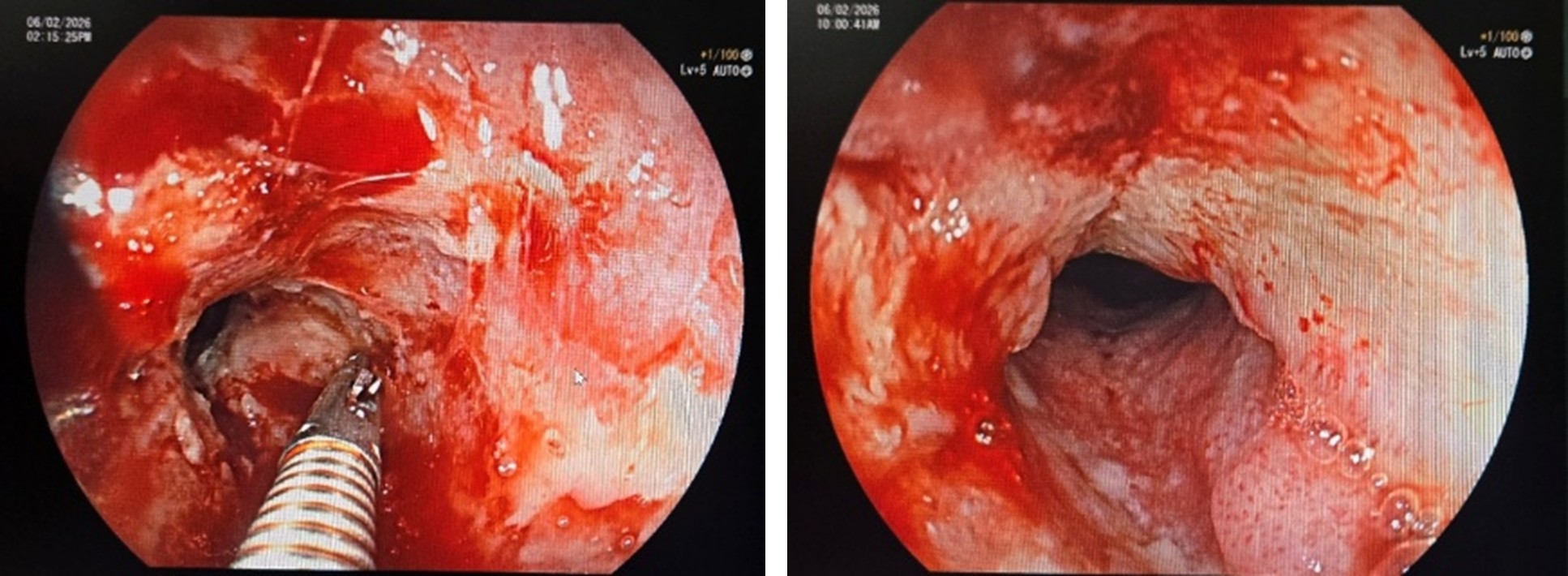
Histopathology: Moderately differentiated squamous cell carcinoma.
CT Chest & Abdomen
- Circumferential wall thickening of the lower esophagus.
- Mild regional lymphadenopathy.
- No distant metastasis.
Post operative CT abdomen

Diagnosis
Moderately differentiated squamous cell carcinoma of the lower esophagus without distant metastasis.
Management
Preoperative Management
Preoperative preparation focused on improving the patient’s nutritional and functional status. Nutritional optimization was initiated due to significant weight loss and reduced oral intake, with dietary supplementation implemented to enhance metabolic reserves. Proton-pump inhibitors were prescribed to reduce gastric acidity and protect the upper gastrointestinal tract. Given the patient’s comorbid hypertension, COPD, and history of cerebrovascular accident, cardiology and pulmonology consultations were obtained for risk stratification and optimization of cardiorespiratory function. A thorough pre-anaesthetic evaluation assessed suitability for general and epidural anaesthesia. Routine laboratory investigations, including haematological and biochemical profiles, were completed to correct any abnormalities prior to surgery.
Intraoperative Management
The patient underwent a minimally invasive esophagectomy using Video-Assisted Thoracoscopic Surgery (VATS) under general anaesthesia supplemented with epidural analgesia. Standard monitoring and positioning were ensured, and the procedure was performed through thoracoscopic and laparoscopic access.
Intraoperative Findings
Thoracoscopic evaluation revealed a proliferative lesion in the mid esophagus, located approximately 5 cm below the carina. Multiple infracarinal and periesophageal lymph nodes were noted. The right lung displayed multiple bullae, with adhesions to the parietal pleura, which were carefully dissected. Examination of the abdominal cavity showed no abnormalities, and all abdominal viscera appeared normal.
Surgical Procedure
The diseased segment of the esophagus was mobilized and resected. The stomach was prepared by mobilization and tabularization to create a gastric conduit suitable for reconstruction. Following mobilization, a gastric pull-up was performed, bringing the conduit into the thoracic cavity. An end-to-end esophagogastric anastomosis was then completed. A feeding jejunostomy tube was inserted to facilitate postoperative enteral nutrition. Haemostasis was ensured, and thoracic and abdominal drains were placed as per standard protocol. The procedure was completed successfully with no intraoperative complications.
Postoperative Management
The patient was transferred to the intensive care unit (ICU) for close monitoring with ventilatory support. Hemodynamic parameters were stable. Intravenous fluids, broad-spectrum antibiotics, and epidural analgesia were initiated. Continuous monitoring of vital signs, urine output, and drain output was maintained.
Postoperative Day 1
The patient was successfully extubated and maintained adequate oxygen saturation on supplemental oxygen. Enteral nutrition through the feeding jejunostomy (FJ) tube was initiated. Respiratory care including chest physiotherapy, incentive spirometry, and nebulization was started. Serum electrolytes were monitored and corrected as required.
Postoperative Day 2
The patient remained hemodynamically stable. Enteral feeds were gradually increased as tolerated. Aggressive pulmonary rehabilitation was continued to prevent postoperative respiratory complications.
Postoperative Day 3
The patient continued to show clinical stability. FJ feeds were well tolerated. Chest physiotherapy and incentive spirometry were continued. Routine monitoring of electrolytes and fluid balance was maintained.
Postoperative Day 4
The cervical drain was removed after satisfactory output and clinical assessment. The patient showed gradual improvement in respiratory status and nutritional tolerance.
Postoperative Day 5
The patient developed high-grade fever. Antibiotic therapy was escalated. Further evaluation was performed to identify the source of infection.
Postoperative Day 6
A contrast enhanced CT scan of the chest and abdomen was performed to rule out an anastomotic leak. The scan showed no evidence of leak but revealed bilateral lung infiltrates with collapse of the right basal lobe. Due to respiratory compromise, the patient was shifted back to the ICU for advanced respiratory care. Broad-spectrum antimicrobial therapy including Colistin and antifungal agents was initiated as per pulmonologist recommendations. Intensive pulmonary rehabilitation was continued.
Postoperative Day 7
The patient showed gradual clinical improvement. Drains were monitored and removed sequentially as per output and clinical condition. Enteral feeding continued with gradual introduction of oral liquids.
Postoperative Day 8
The patient experienced another febrile spike. The central venous catheter was removed, and blood cultures were obtained. Oral feeding was tolerated well along with FJ supplementation.
Postoperative Day 9
No further fever episodes were noted. The intercostal drain (ICD) was removed. The patient demonstrated significant clinical improvement with stable vital signs and adequate respiratory function.
Nursing Management
Airway and Respiratory Management
- Continuously monitored the airway patency and respiratory status.
- Administrated the oxygen therapy as prescribed.
- Encouraged regular respiratory exercises, including.
-
- Incentive spirometry.
- Chest physiotherapy.
- Nebulization.
- Positioned the patient in semi-Fowler’s to promote lung expansion and reduce aspiration risk.
Pain Management
- Monitored the pain intensity using appropriate pain scales.
- Administered epidural and intravenous analgesics as prescribed.
- Ensured the adequate pain control to facilitate early ambulation and effective breathing exercises.
Fluid, Nutrition, and Drain Management
- Monitored Intake and output hourly.
- Feeding jejunostomy (FJ) feeds were carefully managed, ensuring accurate administration of prescribed nutrition, routine flushing to maintain patency, and vigilant measures to prevent tube blockage.
- Monitored drainage output from neck, thoracic, and abdominal drains, reporting abnormalities promptly.
Prevention of Pulmonary Complications
- Early mobilization was encouraged within the patient’s tolerance frequent repositioning to prevent atelectasis.
- Ensured proper technique in breathing exercises.
- Monitored the signs of respiratory distress such as tachypnea, desaturation, or increased work of breathing.
Wound Care and Infection Prevention
- Strict aseptic techniques were adhered to while handling surgical wounds, drains, and the FJ tube.
- Monitored any signs of infection such as fever, redness, discharge, foul odour, or increased pain.
- Performed routine dressing changes as per protocol.
Nutritional Support
- A gradual progression from jejunostomy feeds to oral liquids and a soft diet was initiated once permitted.
- Ensured adequate caloric and protein intake to promote healing.
- Provided dietary counselling to avoid reflux-triggering and irritant foods.
Patient and Family Education
- Instructions regarding home care of the feeding jejunostomy tube, including cleaning, flushing, and recognizing signs of complications, were provided.
- Educated about small, frequent meals and upright posture after feeding.
- Taught about early warning signs requiring immediate medical attention.
- Reinforced medication adherence and follow-up visits.
Outcome
The patient demonstrated progressive clinical improvement following initial postoperative respiratory complications. He gradually tolerated both oral and jejunostomy feeds without difficulty and maintained stable hemodynamic parameters throughout the remainder of his hospital stay. Serial monitoring showed no recurrence of fever, and respiratory function improved significantly with consistent physiotherapy and pulmonary rehabilitation measures.
By the time of discharge, the patient was clinically stable, ambulating with minimal assistance, and maintaining adequate nutritional intake. He was discharged with instructions to continue intravenous antibiotics at home along with scheduled follow-up appointments for surgical, nutritional, and pulmonary evaluation.
Discharge Advice
The patient was discharged in a stable clinical condition after demonstrating satisfactory recovery and tolerance to both oral and jejunostomy feeding. Detailed discharge instructions were provided to ensure continuity of care and to support recovery at home.
Medications
At the time of discharge, the patient was advised to continue the prescribed medications, including intravenous antibiotics for completion of the treatment course, analgesics for pain control, bronchodilators for respiratory support, and previously prescribed medications for comorbid conditions such as antihypertensives and anticoagulants.
Dietary Advice
The patient was instructed to follow a structured dietary regimen consisting of small and frequent meals with a soft, high-protein diet to promote healing and maintain adequate nutritional status. Foods that could cause gastric irritation or reflux, including spicy foods, fried items, carbonated beverages, and alcohol, were advised to be avoided. The patient was also counselled to maintain an upright position for at least 30 minutes after meals to reduce the risk of reflux and aspiration.
Follow-Up
Regular follow-up visits were scheduled to monitor recovery and assess for potential complications. The patient was advised to attend follow-up appointments in the surgical outpatient department for postoperative evaluation. Additional consultations with a nutritionist were recommended to ensure adequate nutritional support, along with pulmonology and oncology reviews for ongoing management and surveillance.
Discussion – Medical Aspects
Esophageal carcinoma remains a significant global health concern, particularly in Asian countries where the incidence of squamous cell carcinoma is relatively high. Squamous cell carcinoma arises from the epithelial lining of the esophagus and is strongly associated with lifestyle-related risk factors such as chronic tobacco use, alcohol consumption, and prolonged mucosal irritation. These factors contribute to progressive cellular dysplasia and malignant transformation of the esophageal mucosa. Progressive dysphagia is the most common presenting symptom and usually indicates luminal narrowing caused by tumour growth. Patients initially have trouble swallowing solid foods, which gradually progresses to difficulty with semi-solid and liquid foods as the disease advances. Associated symptoms may include weight loss, regurgitation of undigested food, retrosternal discomfort, and nutritional deficiencies due to reduced oral intake. In recent years, minimally invasive surgical techniques have significantly improved the management of esophageal malignancies. Video-Assisted Thoracoscopic Surgery (VATS) esophagectomy has emerged as an effective alternative to conventional open esophagectomy. Compared with open surgery, minimally invasive approaches provide several benefits, including reduced postoperative pain, decreased pulmonary complications, improved visualization of mediastinal structures, shorter hospital stay, and faster postoperative recovery. When performed in experienced centres, VATS esophagectomy can achieve comparable oncological outcomes while improving overall patient recovery.
For patients with localized esophageal cancer without evidence of distant metastasis, surgical resection remains the cornerstone of curative treatment. Adequate lymph node dissection during esophagectomy is essential for accurate staging and improved oncological control. Early diagnosis and timely surgical intervention significantly influence prognosis and long-term survival. The present case also highlights the influence of comorbid conditions such as chronic obstructive pulmonary disease (COPD), hypertension, and previous cerebrovascular accident (CVA) on perioperative and postoperative outcomes. These comorbidities increase the risk of respiratory complications, delayed recovery, and postoperative morbidity. Therefore, careful preoperative assessment, multidisciplinary collaboration, and vigilant postoperative monitoring are crucial in optimizing patient outcomes.
Discussion – Nursing Aspects
Nursing care is an essential component of the perioperative management of patients undergoing esophagectomy, as these individuals are at high risk for respiratory, nutritional, and postoperative surgical complications. Effective nursing interventions directly influence patient outcomes by ensuring early detection of complications, optimizing recovery, and promoting long-term self-care. One of the primary responsibilities of nursing staff is the early identification of postoperative complications. Vigilant monitoring for signs of anastomotic leak such as tachycardia, fever, increased drain output, or respiratory distress is crucial, as timely recognition can significantly reduce morbidity and mortality. Similarly, prompt identification of symptoms of sepsis or respiratory compromise enables rapid clinical intervention and improved outcomes. Respiratory care is another cornerstone of postoperative nursing management in esophagectomy patients. Due to thoracic involvement, these patients are predisposed to pulmonary complications such as atelectasis, pneumonia, and lung collapse. Nurses play a critical role in implementing pulmonary health measures, including chest physiotherapy, nebulization, incentive spirometry, and encouraging early mobilization to maintain optimal lung function and prevent respiratory deterioration.
Nutritional management is equally significant, as esophagectomy patients often experience impaired oral intake and increased metabolic demands during recovery. The use of feeding jejunostomy (FJ) requires meticulous nursing oversight to ensure adequate caloric and protein intake, prevent tube blockage, and maintain gastrointestinal function. Ongoing assessment and adjustment of feeding regimens support effective wound healing and overall recovery. Pain management remains central to enabling adequate ventilation and early ambulation. Effective control of postoperative pain through epidural, intravenous, or oral analgesics supports respiratory effort, reduces the risk of pulmonary complications, and enhances patient comfort.
Patient and family education forms an integral part of nursing care. Instruction on home care of the FJ tube, safe dietary progression, medication adherence, and recognition of early warning signs empowers patients to participate actively in their recovery and reduces the likelihood of readmission.
Conclusion
Esophageal squamous cell carcinoma remains a challenging malignancy that requires timely diagnosis and a well-coordinated multidisciplinary approach for effective management. Early recognition of symptoms such as progressive dysphagia allows for prompt diagnostic evaluation and intervention, which are critical in improving patient outcomes. Minimally invasive esophagectomy using Video-Assisted Thoracoscopic Surgery (VATS) has emerged as a safe and effective surgical technique for patients with localized disease. Compared with conventional open surgery, it offers advantages such as reduced postoperative pain, lower risk of pulmonary complications, shorter hospital stays, and faster recovery while maintaining satisfactory oncological outcomes. Furthermore, successful management of esophageal carcinoma extends beyond the surgical procedure. Comprehensive postoperative care including vigilant monitoring for complications, effective respiratory rehabilitation, appropriate nutritional support, and dedicated nursing management plays a vital role in ensuring optimal recovery. This case highlights the significance of an integrated, patient centred approach involving surgeons, physicians, nurses, and allied healthcare professionals in the management of esophageal carcinoma. Such coordinated care is essential for improving recovery, minimizing complications, and enhancing the overall quality of life for patients undergoing esophagectomy.
