Poly trauma patient care: A nursing approach
Veena M1*, Shwetha H K 2, Shalini H S3, Vijayakumari4
1Nursing In charge, Kauvery Hospital, Electronic City, Bangalore
2Nursing MOD, Kauvery Hospital, Electronic City, Bangalore
3CNO, Kauvery Hospital, Electronic City, Bangalore
4Nurse Educator, Kauvery Hospital, Electronic City, Bangalore
Abstract
Poly trauma care evolved from military conflicts, particularly during World War 1 & World War 2 where soldiers suffered multiple injuries. The term poly trauma gained prominence during the Vietnam war. Civil-A trauma care advised in the 1970s-80s with ATLS (advanced trauma life support) protocols. Today, poly trauma management involves multidisciplinary teams, focusing on rapid assessment, stabilization, & rehabilitation Poly trauma, also known as multiple traumas, refers to injuries involving multiple body systems or organs, often resulting from high-impact events like road traffic accidents, falls, or violence. Polytrauma is when a patient has sustained multiple injuries, some of which may cause significant disability and may be life-threatening. Worldwide the most common cause of polytrauma is motor vehicle accidents; other causes include suicide and homicide attempts. This activity reviews the evaluation and initial management of the polytraumatized patient and highlights the role of interprofessional team members in collaborating to provide well-coordinated care and enhance patient outcomes. Polytrauma is a major cause of morbidity and mortality in developed and developing countries. This study aims to assess the prevalence and outcome of polytrauma patients, in a tertiary care hospital. Effective nursing care is crucial in managing poly trauma patients, requiring a comprehensive approach to address life-threatening injuries, prevent complication, promote recovery.
Key words: Polytrauma; Tachycardia; Retroperitoneum
Introduction
Poly trauma, also known as multiple traumas, refers to injuries involving multiple body parts or organs, often life-threatening & requiring immediate medical attention. Poly trauma is typically defined as an injury severity score (ISS)>15, indicating significant trauma with potential for organ dysfunction or failure. Worldwide, 16,000 people die every day because of injury. Polytrauma is a combined trauma, in which there are two or more severe injuries that affect at least two anatomical regions; rarely, two or more severe injuries in one anatomic area, whereas at least one of these is life-threatening.[2] Polytrauma is a major cause of morbidity and mortality in developed and developing countries. Trauma is still the leading cause of death and disability in children and young adults.
Case presentation
A 11-year-old female patient presented to the ER with the history of RTA (2-wheeler vs Lorry), near Bangalore. She had sustained degloving injury lower back, right side of abdomen / Right thigh. No head injury / seizure/ ENT bleed/ vomiting. The primary survey follows the ABCDE system that includes assessment and management of Airway, Breathing, Circulation, Disability, and Exposure has been done and initiated the treatment as per ATLS Protocol. Hence, the Patient admitted for further management.
Clinical examination
On arrival:
11 years / Female, average built.
| Pulse | 172 /min. |
|---|---|
| Blood Pressure | 80/50mmHg, |
| Respiratory Rate | 32/min. |
| Temp | Afebrile. |
| SpO2 | 76% on RA. |
| Respiratory System | Bilateral normal vesicular breath sounds present. |
| Cardiovascular System | S1 S2 +, no murmur. |
| Abdomen | Soft, tenderness present. |
| Central Nervous System | Child was restless, GCS: E4V5M6. |
Local examination: Degloving Injury Right Lower Abdomen, Flank, Lower Back and Thigh.
Course in the hospital
11 years, Female was presented with above mentioned history. On arrival at ER, her GCS was E4V5M6, tachycardia, BP: 80/50mmHg, Spo2: 76% in room air. In view of restless and hemodynamic instability. Child was intubated and put on mechanical ventilation. She was evaluated with CT whole body (Trauma Protocol), CT Brain showed Small hemorrhagic foci in the right suprasylvian frontal lobe. ET Tube noted in situ. CT Chest report showed Posterior diaphragmatic tear on the left side for 50 x 40 mm with herniation of the fundus and body of the stomach with greater omentum. Moderate left pleural effusion with basal collapse consolidation. Right lower lobe collapse consolidation sparing the anterior segment. Small ground-glass attenuation in the left upper lobe. Mild deviation of trachea to the right side due to mass effect. Fracture posterior rib of left 11th rib. Suspicious fracture of left 11th/12th posterior rib. CT abdomen pelvis report AAST Grade. Laceration with devascularization of the upper and mid pole of the left kidney with no contrast opacification beyond the upper pole hilar vessels. Attenuation of the draining veins noted. Small perinephric hematoma. Bowel/Mesentery/Omentum: Stomach appears displaced cranially & posteriorly into the posterior mediastinum with tear in the left diaphragm. Relative flattening of the IVC noted – Secondary to Volume Depletion. Extraluminal air pocket noted along the posterior aspect of pancreatic tail (Retroperitoneum) suspecting Pneumoperitoneum. Air pockets along the anterior and posterior abdominal wall with large laceration along the right upper thigh and groin. Fracture left sacral ala. Child had hematuria, urologist opinion was obtained and was advised to managed conservatively
Child was shifted to ICU on intubation and started on supportive medications blood products arranged and adequately resuscitation. Parents were counselled regarding the Major Degloving Injury of Right Lower Abdomen, Flank, Lower Back and Thigh, hemopneumothorax and extensive soft tissue injury, Diaphragmatic injury and requirement of emergency surgical procedure. After obtaining informed consent, child was taken up for Major Wound Debridement local flap with VAC under General anesthesia. Post operatively she was shifted to ICU with ventilatory support, IV antibiotics, fentanyl infusion, IV fluids and sedatives. She also received blood product transfusion (Total 2 PRBC, 1FFP, 1RDP). CTVS Team opinion was taken on the left side ICD was inserted in ICU. Surgical Gastro-opinion was taken in view of rupture of left crura of diaphragm with herniation of stomach and patient was shifted to OT for Diagnostic Laparoscopy + Traumatic Diaphragmatic Repair + Gastropexy under General anesthesia. Post procedure she was shifted to ICU for further management. She was closely monitored by Pediatric intensivist team along with Surgery team.
Child was weaned from ventilator, antibiotics escalated accordingly PICU Team, Surgical Gastro, CTVS Team, Critical Care Team were constantly involved in management of the child. A Bronchoscopy was done and BAL sample sent which was negative. She received 1-unit PRBC with a view to dropping Hemoglobin. Patients were extubated and connected to facemask and NIV. Nephrologist opinion was taken in view of deranged creatinine and advised followed. Left renal ischemic injury managed conservatively. CECT abdomen done which showed laceration with devascularization of the upper and mid pole of the left kidney. Blood and urine culture were negative. USG abdomen and pelvis report showed normal morphology of left kidney with no perinephric collection / hematoma.
Urologist opinion was sought in view of USG findings and advised for CT renal Angiogram once stable. In view of discoloration of degloved skin patient was patient was planned for debridement. After obtaining informed consent patient underwent Major Wound Debridement and VAC. Post operative stay was uneventful. Orthopedician opinion was sought in view of left pubic rami fracture/ Left sacral ala and advised for conservative management. Serial follow up of lab report were done. Right ICD removed. CT renal angiogram report showed Thrombosed upper and mid segmental renal artery branches on the left side. Thrombosed upper segmental renal vein beyond hilum on the left side. Bulky-appearing left upper and mid poles with perinephric fat stranding – Laceration with Ischemia. Disruption of the upper minor and major calyces with no contrast opacification in the delayed scans (Upper Major Calyceal Cut-off). Kidney injury was managed conservatively and hematuria resolved.
Next, patients underwent Wound Debridement, TFL flap for exposed iliac crest (right VAC) under GA. Post procedure stay was uneventful and patient underwent Wound Debridement / SSG with VAC under GA. Post procedure stay uneventful. Patients were managed with IV fluids, antibiotics, analgesics, antacids, nebulization, diuretics and other supportive. Check dressing of skin graft done. Grafts are found to be healthy. It had been explained that children will need to dress under anesthesia after 5 days. Explained risk of infection / seroma, need for further procedure depending on healing. Patient remained hemodynamically stable and she is being discharged in stable condition.
Surgical details
Major wound debridement local flap with VAC
- Peripheral pulses are feeble in upper limb; lower limb pulses are not felt but doppler signals present due to hypotension.
- There is transverse laceration in right lower abdomen extending from hypogastrium to right flank.
- Skin is degloved extending to xiphisternum level in right half of abdomen and across flank to involving lower back across midline posteriorly in lower back.
- There is deglove of upper anterior thigh extending laterally to involve degloving of gluteal region, lateral and posterior thigh in upper half.
- Gluteal muscle is avulsed from insertion and proximal part is non-viable.
Procedure
- Wound debrided, non-viable, muscle, skin and degloved subcutaneous fat debrided.
- Part of wound covered with local degloved flap.
- Residual raw area in right right iliac region flanks and upper thigh covered with VAC.
- Hemostasis maintained.
It has been explained to parents that the child will require multiple procedures to inform them of flap / skin graft / prolonged ICU stay.
1. Diagnostic Laparoscopy + Traumatic Diaphragmatic Repair + Gastropexy
Findings
- RTA with crush injury.
- Left hemopneumothorax with ICD in situ.
- Left hemidiaphragm injury with tear of left crura of diaphragm with herniation of stomach into left hemithorax.
2. Major wound debridement and VAC
Findings: Raw area in Right iliac fossa, upper thigh and flank. Surrounding deglove of skin and soft tissue extending to upper thigh laterally and posteriorly. Degloving involving right gluteal region, lower back, lower chest on right side. There is further necrosis of degloved skin.
Procedure: Under GA, wound debrided necrotic skin, subcutaneous tissue debrided. Partially avulsed gluteal muscles are also necrotic and was debrided. Hemostasis achieved. VAC applied to raw area. Plan for further procedure after 72 hours. Swab sent for pus culture sensitivity.
3. Wound debridement, TFL flap for exposed iliac crest (right VAC)
Procedure: Under GA, the wound in (right iliac fossa/ flank / upper thigh debrided. Exposed iliac crest covered with TFL flap. VAC dressing done.
4. Wound debridement / SSG with VAC
Procedure
- The wounds in right lower back, flank, right iliac region and upper thigh.
- The degloved skin in lower back and upper thigh yet to adhere completed.
- Raw area covered with SSG.
- Dressing done VAC applied.
- Drain kept in situ.
5. Wound dressing in graft + Seroma drainage
Procedure
Under sedation skin graft in Right flank and right lower abdomen inspected graft plate is good except over right iliac crest. There is seroma collection in degloved region of upper thigh and lower back. Wound dressing done, seroma drainage. Drain kept at site of seroma. Graft dressing done.
6.Wound Debridement Split Skin Graft – Right Flank. Removal of Retained Stapler
Procedure
Under General Anesthesia wound debrided in the right flank, retained stapler removed & residual raw area grafted.
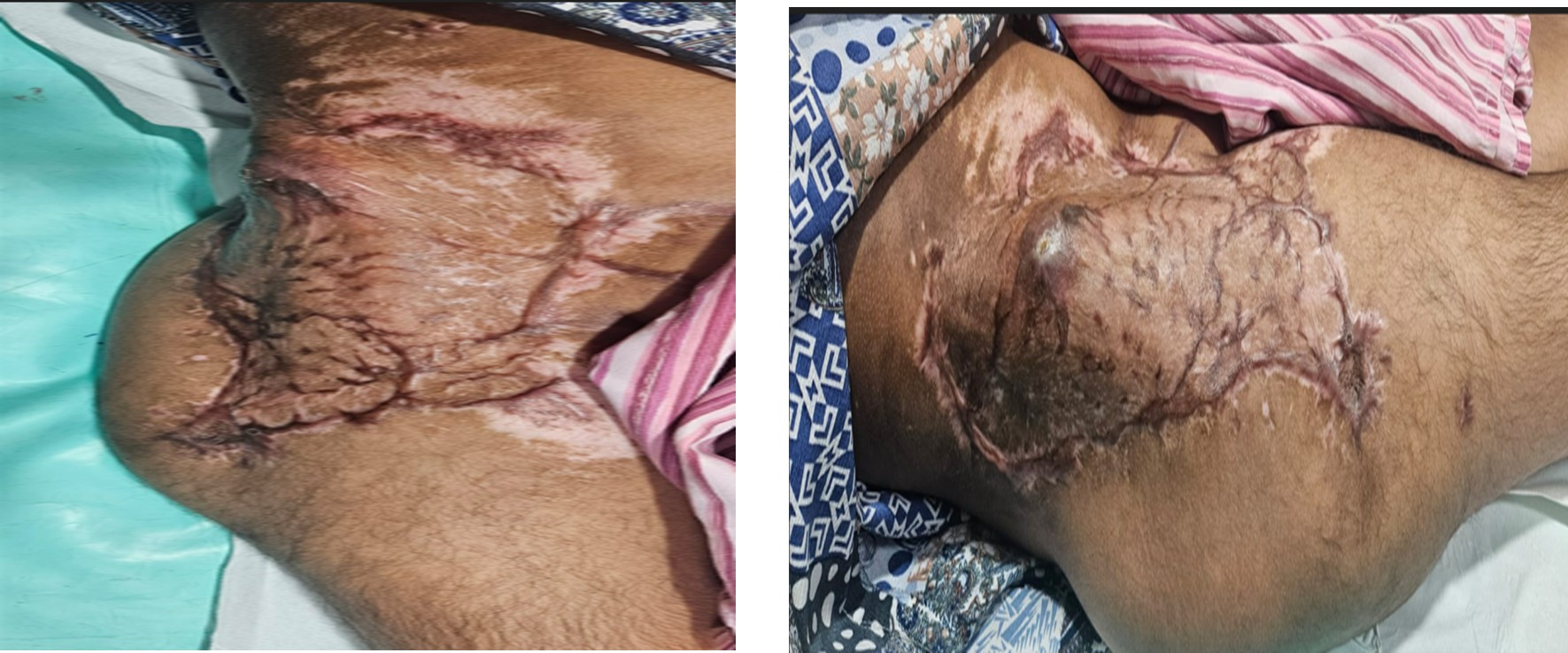
Poly Trauma Wound

Follow up Phase

Recovery phase
Discussion
The core discussion points for managing a polytrauma patient according to Advanced Trauma Life support (ATLS) guidelines center on a structured, prioritized approach to immediately identify and treat life-threatening injuries. This process is divided into primary survey, resuscitation efforts, secondary survey, and definitive care. Poly trauma injury to >2 body systems, at least one of which is life-threatening, resulting from a single traumatic event.
Goals of ATLS
Primary survey (ABCDE)-Life saving phase
- Airway with cervical spine protection
Assess patency(talking=patent)
Look for
Facial trauma, blood, vomitus, Stridor, hoarseness
Interventions
- Jaw thrust, suction
- Oropharyngeal/nasopharyngeal airway
- Endotracheal intubation if needed
- C-spine immobilization mandatory
B-Breathing and ventilation
- Inspect, palpate, percuss, auscultate
Look for immediate life-threatening injuries:
- Tension pneumothorax
- Open pneumothorax
- Massive hemothorax
- Flail chest
Interventions
- High flow oxygen
- Needle decompression
- Chest tube insertion
C-Circulation with hemorrhage control
Assess
- Pulse, BP, capillary refill
- Skin color and temperature
Control external bleeding
- Direct pressure
- Tourniquet
Establish
- 2 large -bore iv lines
- Blood sampling
Fluid resuscitation: Crystalloids-blood (MTP if required)
Identify sources of bleeding: Chest, abdomen, pelvic, long bones
Disability (Neurological status)
- GCS assessment
- Pupils (size, symmetry, reaction)
- Check blood glucose
- Rapid lateralizing signs
D-Exposure and Environmental control
- Completely expose patient
- Look for hidden injuries
Prevent hypothermia: Warm blankets, Warm iv fluids
Adjuncts to primary survey
- Pulse oximetry
- ECG monitoring
- ABG
- FAST / e-FAST
- Portable X-ray (chest, pelvis)
Secondary survey-head-to-toe evaluation Performed only after stabiliztion
Complete history (AMPLE)
- Allergies
- Medications
- Past illness/pregnancy
- Last meal
- Events leading to injury
Detailed examination
- Head & neck
- Chest
- Abdomen
- Pelvis
- Limbs
- Spine
Imaging: CT scan (trauma protocol) if stable
Definitive care
- Surgical intervention as required
- ICU admission if indicated
- Damage control surgery
- Multidisciplinary management
Key principles
- Primary survey may be repeated multiple times
- Life over limb
- Do not delay treatment for investigations
- Assume cervical spine injury until ruled out
- Early haemorrhage control saves lives
Common causes of death in polytrauma
- Haemorrhage
- Traumatic brain injury
- Sepsis/MOF (late)
Nursing management
Nursing management for polytrauma focuses on rapid, systematic assessment (ABCDEs), immediate life-saving interventions, continuous monitoring, multisystem support (respiratory, cardiac, renal), pain management, and advocating for the patient within a multidisciplinary team, using protocols like ATLS to address critical injuries first and prevent complications like shock or organ failure. Key actions include securing airways, controlling bleeding, managing fluids, assessing neurological status (GCS, pupils), preventing hypothermia, administering analgesics, and ensuring clear communication.
Key nursing responsibilities
Rapid Primary Survey (ABCDEs)
Airway: Check patency, suction, manage artificial airways, ensure adequate ventilation.
Breathing: Assess respiratory rate, oxygenation, chest movement; identify pneumothorax/hemothorax.
Circulation: Control hemorrhage, assess pulse, BP, perfusion; implement damage control resuscitation (warm fluids, lower BP targets).
Disability: Reassess GCS, pupils; check neurological deficits.
Exposure/Environment: Remove clothing to find injuries, maintain normothermia (warm blankets).
Resuscitation & monitoring
- Establish IV access and initiate warmed fluid/blood product administration.
- Continuous vital sign monitoring (BP, HR, SpO2, ECG).
- Insert/manage lines (central, arterial) and life-support equipment.
Pain & Anxiety management:
- Administer prescribed IV analgesics (titrate opioids) to reduce pain and anxiety.
- Communicate with the patient to reduce fear.
Multisystem support
- Manage ventilators, fluid balance, electrolyte levels.
- Collect blood for labs (CBC, type & crossmatch, cardiac markers).
Secondary survey & advocacy
- Assist with comprehensive head-to-the-respondence assessment to find all injuries.
- Act as the patient’s advocate, voicing concerns about pain, comfort, and needs to the trauma team.
Communication & documentation:
- Utilize structured handoffs (e.g., SBAR).
- Ensure clear, rapid communication among the multidisciplinary team.
Preventing complications
Prevent hypothermia (warming fluids, blankets) and monitor for shock, sepsis, and organ dysfunction.
Conclusion
The conclusion of a polytrauma presentation emphasizes that effective management is a complex, multidisciplinary effort crucial for patient survival and long-term recovery. While immediate life-saving interventions in the “golden hour” are vital, the full spectrum of care, including rehabilitation and psychological support, ultimately determines the patient’s long-term quality of life.
Key takeaways
Complexity and Urgency: Polytrauma remains a leading cause of death and disability worldwide, requiring immediate, coordinated action by a specialized, interprofessional team (trauma surgeons, orthopedists, neurosurgeons, nurses, etc.).
Standardized Protocols: Adherence to structured algorithms like Advanced Trauma Life Support (ATLS) and Pre-Hospital Trauma Life Support (PHTLS) are essential for prioritizing life-threatening injuries (e.g., airway, breathing, circulation) and improving outcomes.
Physiological management: Key to survival is managing the “lethal triad” of acidosis, hypothermia, and coagulopathy through damage control resuscitation (DCR), which involves judicious fluid administration and balanced blood transfusions.
Balancing interventions: A critical decision point in polytrauma care is the timing of definitive surgeries. The choice between Early Total Care (ETC) for stable patients and Damage Control Orthopedics (DCO) for unstable patients depends on the individual’s physiological status to avoid a “second hit” or systemic inflammatory response syndrome (SIRS).
Long-term recovery: Survival is only the first step. Recovery often takes years and involves comprehensive rehabilitation, including physical, occupational, and psychological support, to address potential long-term physical, cognitive, and emotional impairments like PTSD.
In sum, continuous advancements in trauma care protocols, team coordination, and rehabilitation strategies are crucial for enhancing survival rates and optimizing functional outcomes for polytrauma patients.
