Emergency laparotomy in a patient with bleeding duodenal ulcer
Sumithra*
Staff Nurse, ICU Department, Kauvery Hospital, Hosur, Tamil Nadu
*Correspondence
Abstract
Upper gastrointestinal bleeding (UGIB) is a potentially life-threatening emergency requiring prompt diagnosis and multidisciplinary management. Peptic ulcer disease remains one of the most common causes of UGIB. Although endoscopic therapy is the primary treatment modality, persistent or recurrent bleeding may necessitate emergency surgical intervention. This case report describes with hematemesis and melena secondary to a bleeding duodenal ulcer (Forrest IIb). Despite initial endoscopic management with bipolar cauterization and adrenaline injection therapy, the patient remained at high risk for recurrent hemorrhage. Emergency exploratory laparotomy with ligation of the bleeding gastroduodenal artery, truncal vagotomy, and feeding jejunostomy was performed. Postoperatively, the patient required intensive monitoring, blood transfusions, nutritional support, and comprehensive nursing care. The patient recovered gradually and was discharged in a stable condition. This report emphasizes the importance of early recognition, prompt surgical intervention, vigilant postoperative care, and multidisciplinary teamwork in managing severe upper gastrointestinal bleeding.
Key words: Upper gastrointestinal bleeding (UGIB); Laparotomy
Introduction
Upper gastrointestinal bleeding (UGIB) is defined as bleeding originating proximal to the ligament of Treitz, involving the oesophagus, stomach, or duodenum. It is a common medical emergency with significant morbidity and mortality. Peptic ulcer disease accounts for nearly 50% of UGIB cases worldwide. Clinical manifestations include hematemesis, coffee-ground vomiting, melena, dizziness, syncope, fatigue, and signs of hypovolemic shock. Although advances in endoscopic haemostatic techniques and proton pump inhibitor therapy have reduced the need for surgery, emergency operative management remains essential in cases of uncontrolled haemorrhage, recurrent bleeding, or failed endoscopic treatment.
Case Presentation
A 33-year-old male was admitted with complaints of one episode of blood-stained vomiting (hematemesis) and multiple episodes of black tarry stools (melena) for one day. The patient also reported generalized weakness and dizziness. The patient was a known case of psoriasis and was on regular treatment.
Relevant Clinical Findings
General Examination
- Conscious, alert, and oriented
- Pallor present
- Signs suggestive of acute blood loss
Vital Signs on Admission
| Parameter | Finding |
|---|---|
| Pulse Rate | 118 beats/min |
| Blood Pressure | 90/60 mmHg |
| Temperature | 98.1°F |
| SpO₂ | 98% on room air |
| GRBS | 200 mg/dL |
Systemic Examination
Cardiovascular System: S1 and S2 heard normally
Respiratory System: Bilateral vesicular breath sounds
Abdominal Examination
- Soft abdomen
- Non-tender
- No guarding or rigidity
Central Nervous System: No focal neurological deficits
Investigations
| Investigations | Pre Op | Post Op |
|---|---|---|
| Hb | 6.3 g/dl | 7.6 g/dl |
| Hemotocrit | 19.8% | 23.9 % |
| WBC | 9550 Cells/Cumm | 8810 Cells/Cumm |
| Platelet | 254000 Lakhs/Cumm | 241000 Lakhs/Cumm |
| Urea | 32.1 mg/dl | 19.2 mg/dl |
| Creatinine | 1.1 mg/dl | 0.7 mg/dl |
| Sodium | 134 mmol/L | 136 mmol/L |
| Potassium | 5.7 mmol/L | 3.7 mmol/L |
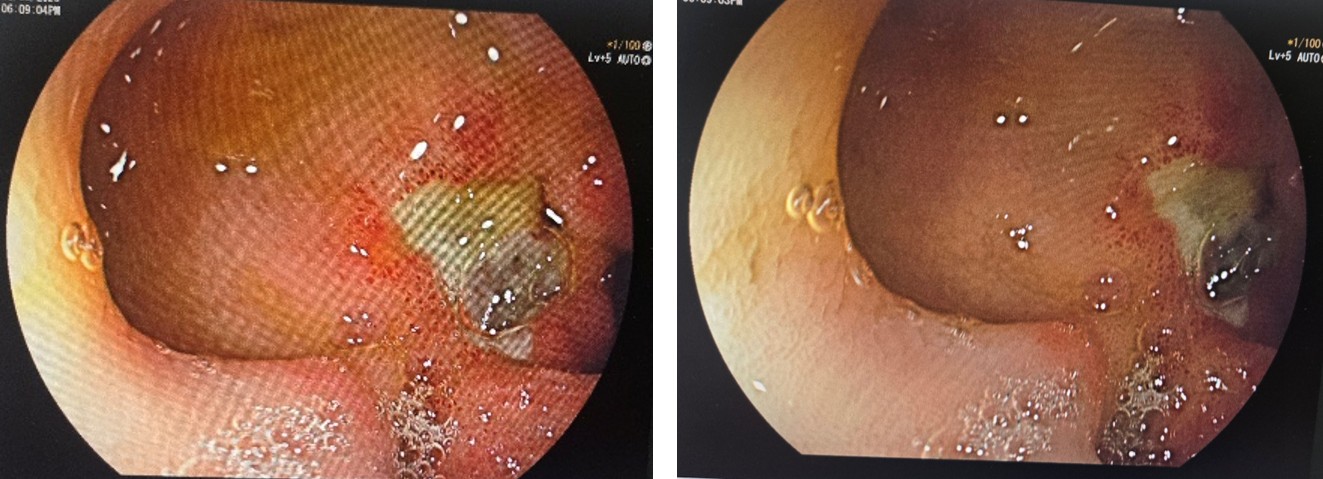
Upper Gastrointestinal Endoscopy Findings
13/03/2026
- Active bleeding identified
- Bipolar cauterization performed
16/03/2026
- Large posterior wall duodenal ulcer
- Adherent clot present
- Evidence of active bleeding
- Adrenaline injection administered in four quadrants
- Classified as Forrest IIb ulcer
Diagnosis: Bleeding Duodenal Ulcer (Forrest IIb) causing Massive Upper Gastrointestinal Bleeding.
Secondary Diagnosis
- Acute blood loss anemia
- Hypovolemic shock secondary to gastrointestinal hemorrhage
Intraoperative Findings
- Large posterior wall duodenal ulcer involving the first part of the duodenum
- Active hemorrhage from the gastroduodenal artery
- Stomach and duodenum filled with blood and clots
- Successful surgical hemostasis achieved
Blood Products Administered
Intraoperatively
- PRBC – 4 Units
- FFP – 4 Units
- Cryoprecipitate – 4 Units
Postoperatively
- PRBC – 2 Units
Postoperative Management
POD 0 (Day of Surgery)
Patient shifted to the Intensive Care Unit (ICU) following emergency exploratory laparotomy with ligation of the bleeding gastroduodenal artery, truncal vagotomy, and feeding jejunostomy. Continuous hemodynamic monitoring initiated. Mechanical ventilation support provided initially, and the patient was subsequently extubated after stabilization. Inotropic support commenced for maintenance of blood pressure and tissue perfusion. Intravenous fluids, proton pump inhibitor infusion, broad-spectrum antibiotics, analgesics, and supportive medications administered. Strict intake and output monitoring maintained. Surgical drain output monitored.
POD 1
Vital signs and hemodynamic parameters monitored closely. Inotropic support gradually tapered according to clinical improvement. Nebulization therapy, chest physiotherapy, and incentive spirometry initiated to prevent pulmonary complications. Intravenous medications and fluid therapy continued. Monitoring for signs of recurrent gastrointestinal bleeding, infection, and postoperative complications performed. Repeat hemoglobin assessment showed 6.3 g/dL. Two units of packed red blood cells (PRBCs) transfused.
POD 2
Hemodynamic status remained stable. Enteral feeding through the feeding jejunostomy initiated in a phased manner. Nutritional tolerance assessed regularly. Electrolyte levels monitored and corrected as required. Respiratory exercises and early mobilization encouraged. Surgical wound and drain site assessed and dressed using aseptic technique.
POD 3
Clinical condition improved significantly. Patient transferred from ICU to the ward. Intravenous medications continued as prescribed. Regular wound inspection and dressing changes performed. Intake and output monitoring continued. Gradual mobilization encouraged. Monitoring for signs of infection, rebleeding, and feeding intolerance continued.
POD 4
Jejunostomy feeding progressively increased according to tolerance. Bowel sounds assessed and gastrointestinal function monitored. Ambulation encouraged with assistance. Laboratory parameters reviewed and electrolyte correction continued if required. Pain managed effectively with prescribed analgesics.
POD 5
Continued clinical improvement observed. Nutritional intake optimized. Respiratory exercises and ambulation continued. No evidence of recurrent hematemesis, melena, or postoperative complications. Surgical wound healing assessed and documented.
POD 6
Patient remained hemodynamically stable. Foley catheter removed following satisfactory urine output and recovery of bladder function. Oral intake gradually advanced. Jejunostomy feeding continued as required. Ongoing monitoring of wound healing and bowel function performed.
POD 7
Patient tolerated normal oral diet without difficulty. No further episodes of hematemesis or melena noted. Repeat hemoglobin level improved to 8.1 g/dL. Independent ambulation achieved. Overall clinical condition remained stable.
POD 8
Abdominal drain removed after minimal drain output and satisfactory recovery. Final assessment confirmed stable vital signs and adequate oral intake. Surgical wound healthy with no signs of infection.
Nursing Management
Hemodynamic Monitoring
- Continuous monitoring of vital signs including heart rate, blood pressure, respiratory rate, temperature, and oxygen saturation.
- Monitored central and peripheral perfusion.
- Assessed for tachycardia, hypotension, pallor, diaphoresis, and altered sensorium.
- Monitored for altered consciousness and risk of aspiration due to hematemesis.
Monitoring for Rebleeding
- Observed for fresh hematemesis, coffee-ground vomiting, or melena.
- Monitored abdominal symptoms and bowel movements.
- Assessed for dizziness, syncope, weakness, and signs of recurrent hemorrhage.
- Recorded color, consistency, and frequency of stools.
Blood Transfusion and Fluid Management
- Administered intravenous fluids as prescribed.
- Assisted with transfusion of packed red blood cells, fresh frozen plasma, and cryoprecipitate.
- Monitored for transfusion reactions.
- Maintained accurate intake and output records.
- Monitored urine output as an indicator of adequate tissue perfusion.
Pain Management
- Assessed pain using standardized pain assessment scales.
- Administered prescribed analgesics.
- Evaluated effectiveness of pain relief measures.
- Encouraged splinting of the abdominal incision during coughing and movement.
Respiratory Care
- Encouraged deep-breathing and coughing exercises.
- Assisted with incentive spirometry.
- Performed chest physiotherapy as indicated.
- Administered nebulization therapy.
- Monitored for signs of atelectasis, pneumonia, or respiratory compromise.
Wound and Drain Care
- Maintained aseptic technique during dressing changes.
- Assessed the surgical incision for redness, swelling, discharge, bleeding, or wound dehiscence.
- Monitored abdominal drain output and characteristics.
- Documented wound healing progress.
Feeding Jejunostomy Care
- Assessed jejunostomy site for infection, leakage, or skin irritation.
- Administered enteral feeds as prescribed.
- Monitored tolerance to feeding, including abdominal distension, nausea, vomiting, and diarrhea.
- Maintained tube patency through appropriate flushing techniques.
Nutritional Management
- Assisted in initiation and progression of jejunostomy feeding.
- Monitored nutritional status and caloric intake.
- Encouraged high-protein and high-fiber diet when oral feeding was resumed.
- Promoted adequate hydration.
Infection Prevention
- Practiced strict hand hygiene and aseptic techniques.
- Administered prescribed antibiotics.
- Monitored for fever and signs of infection.
Deep Vein Thrombosis Prevention
- Encouraged early ambulation.
- Assisted with range-of-motion exercises.
- Promoted adequate hydration.
Gastrointestinal Monitoring
- Assessed bowel sounds regularly.
- Monitored return of bowel function.
- Observed for abdominal distension, nausea, vomiting, and constipation.
Patient and Family Education
- Educated regarding medication adherence.
- Explained dietary modifications and lifestyle changes.
- Advised avoidance of smoking, alcohol consumption, and unnecessary NSAID use.
- Instructed regarding proper wound care and personal hygiene.
- Educated about warning signs requiring immediate medical attention, including:
- Hematemesis
- Melena
- Severe abdominal pain
- Dizziness or syncope
- Fever
- Signs of wound infection
Psychological Support
- Provided emotional support to reduce anxiety and fear.
- Encouraged patient and family participation in care.
- Addressed concerns regarding surgery, recovery, and long-term prognosis.
- Promoted confidence and adherence to the treatment plan.
Outcome
The patient demonstrated a favourable clinical outcome following emergency laparotomy and comprehensive postoperative management. Hemodynamic stability was gradually achieved, allowing successful extubation and discontinuation of inotropic support. No further episodes of hematemesis or melena were observed during the hospital stay, indicating effective control of the gastrointestinal hemorrhage. Serial laboratory investigations showed improvement in hemoglobin levels from 6.3 g/dL to 8.1 g/dL following blood transfusion and supportive therapy. The patient tolerated enteral nutrition through the feeding jejunostomy, followed by a gradual transition to oral feeding without complications. Normal bowel function was restored, and the surgical wound healed satisfactorily without evidence of infection or dehiscence. The patient remained clinically stable throughout the remainder of the hospitalization and was discharged in good general condition with appropriate medications, lifestyle advice, and follow-up instructions.
Discharge
The patient was discharged on postoperative day 8 in a stable condition. At the time of discharge, he was conscious, alert, and oriented, afebrile, hemodynamically stable, tolerating oral feeds well, and passing stools normally without any further episodes of hematemesis or melena. He was prescribed Tab. Nexpro 40 mg for gastric acid suppression, Tab. Ketoflam P 100/325 mg as needed for pain relief, Tab. Zincovit as nutritional supplementation, and Peptamen powder (4 scoops daily) to support nutritional recovery. The patient was advised to avoid heavy lifting and abdominal straining for 6–8 weeks, maintain a high-fiber diet with adequate hydration, adhere to wound care instructions, and abstain from smoking, alcohol consumption, and unnecessary use of NSAIDs. The importance of compliance with medications and follow-up appointments was emphasized. He was advised to undergo scheduled gastroenterology reviews and periodic endoscopic surveillance as recommended. The patient and family were educated regarding the warning signs of recurrent gastrointestinal bleeding, including hematemesis, melena, dizziness, and severe weakness, and were instructed to seek immediate medical attention should any of these symptoms occur.
Discussion – Medical Aspects
Bleeding duodenal ulcer remains one of the most common causes of severe UGIB. Posterior duodenal ulcers are particularly dangerous because of their proximity to the gastroduodenal artery, which can result in massive hemorrhage. Endoscopic therapy is the first-line treatment; however, patients with For rest IIb lesions remain at significant risk of recurrent bleeding. In this patient, despite endoscopic interventions, the risk of rebleeding persisted, necessitating emergency surgical management. Surgical ligation of the bleeding vessel effectively controlled hemorrhage. Truncal vagotomy was additionally performed to reduce gastric acid secretion and decrease future ulcer recurrence. Timely surgery, aggressive transfusion support, and intensive postoperative care contributed significantly to the favourable outcome.
Discussion – Nursing Aspects
Nursing care played a vital role throughout the patient’s treatment and recovery. Early recognition of hypovolemia, frequent monitoring of vital signs, and rapid initiation of resuscitative measures helped stabilize the patient. Postoperatively, nursing interventions focused on hemodynamic monitoring, pain management, prevention of respiratory complications, wound care, nutritional support, and patient education. Continuous observation for recurrent bleeding and postoperative complications facilitated early intervention when necessary. Education regarding medication adherence, dietary modifications, lifestyle changes, and warning signs of rebleeding empowered the patient and family to participate actively in long-term care. The comprehensive nursing approach contributed substantially to the patient’s recovery and prevention of complications.
Conclusion
This case demonstrates the importance of prompt diagnosis and multidisciplinary management in patients presenting with massive upper gastrointestinal bleeding secondary to a bleeding duodenal ulcer. Although endoscopic therapy remains the cornerstone of treatment, emergency laparotomy continues to be a lifesaving intervention when bleeding persists or recurs. Comprehensive postoperative monitoring, timely medical and surgical management, and evidence-based nursing care are crucial for successful patient outcomes. Early recognition, coordinated teamwork, and patient education remain key factors in reducing morbidity and preventing recurrence.
