Blunt thoracoabdominal trauma with rib fractures and muscle laceration: A case report
Mageshwari*
ICU In charge, Kauvery Hospital, Hosur, Tamil Nadu
*Correspondence
Abstract
Blunt thoracic trauma is a major contributor to morbidity and mortality, frequently resulting from road traffic accidents. Multiple rib fractures can compromise ventilation and significantly increase the risk of complications such as pneumothorax, haemothorax, and pulmonary contusion. Muscle lacerations further intensify tissue damage, leading to bleeding, inflammation, and impaired chest wall stability.
Key words: Blunt thoracic trauma; Road traffic accident (RTA);
Introduction
Blunt thoracic trauma is commonly encountered following road traffic accidents, falls, and direct impact injuries. Injuries such as rib fractures, lung contusions, and soft tissue trauma can severely compromise respiratory function. Multiple rib fractures contribute to severe pain, splinting of the chest, and decreased ventilation, predisposing the patient to respiratory failure. In addition, abdominal organ involvement such as liver or kidney injury further complicates the clinical picture. Prompt recognition, appropriate imaging, early stabilization, and coordinated medical and nursing interventions significantly improve patient outcomes.
Case Presentation
A 29-year-old male was brought to the emergency department after a road traffic accident (RTA). He sustained injuries to the right chest, abdomen, and right thigh and presented with severe pain over the right chest wall and right thigh. He was initially treated at a nearby hospital and referred for advanced management.
Past Medical History
- No known comorbidities
- No previous surgeries
- No medication or allergy history
Clinical Findings
Neurological Status (On Admission)
- Drowsy but obeying commands
- Respiratory distress present
General Examination
Drowsy, responding to verbal commands
Vital signs:
| BP | 130/90 mmHg |
| PR | 120 beats/min |
| RR | 40 breaths/min |
| Temperature | 98 °F |
| SpO2 | 89% on RA |
| CVS | S1S2 ( + ) |
| RS | BAE ( + ) |
| P/A | Soft |
| CNS | NFND |
Local Examination
Chest Examination
- Bruising and swelling over right chest wall
- Tenderness and crepitus over multiple right ribs
- Reduced chest expansion on the right
- Decreased breath sounds on the right
Abdominal Examination
- Tenderness in right upper quadrant
- Guarding present
- No abdominal distension
Soft tissue findings
- Right chest wall muscle laceration
- Localized swelling with suspected hematoma
Injuries identified
- Right chest wall: Open crush injury with exposed soft tissue (20 × 7 × 5 cm)
- Right thigh: Puncture wound (1 × 3 × 0.5 cm)
- Left thumb: Abrasion (2 × 1 cm)
Lab results
| Investigation | Pre Op | Post Op |
|---|---|---|
| Hb | 13.9 g/dL | 9.9 g/dL |
| PCV | 41.0 % | 28.5 % |
| WBC count | 20650 cells/mm3 | 8500 cells/ mm3 |
| Platelet | 357000 Lakhs/ mm3 | 248000 Lakhs/Cumm |
| Ph | 7.35 | 7.49 |
| PCO2 | 37 mmHg | 30 mmHg |
| PO2 | 114 mmHg | 132 mmHg |
| HCO3 | 20.4 mmol/L | 22.9 mmol/L |
| Sr. Urea | 19.1 mg/dL | - |
| Sr. Creatinine | 0.8 mg/dL | - |
| Na+ | 140 mmol/L | 136 mmol/L |
| K+ | 4.1 mmol/L | 3.6 mmol/L |
| INR | 1.06 | - |
Investigations
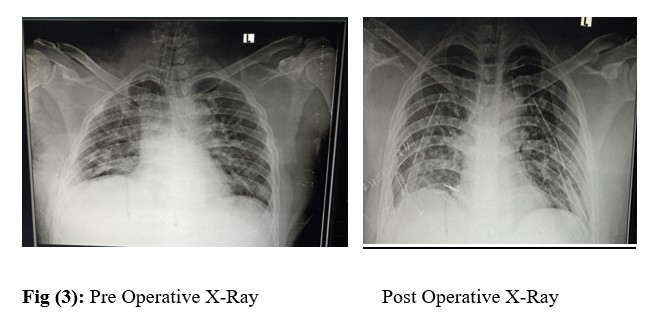
| Chest X-ray | Multiple right rib fractures (5th, 6th, 7th ribs) |
| Ultrasound Abdomen | Suspicion of internal injury |
| CT Chest & Abdomen | Multiple right-sided rib fractures, Grade III liver laceration involving both lobes , Mild right perinephric hematoma , Right kidney contusion (lower pole) |
| CT Brain | No intracranial haemorrhage |
| Blood Tests | CBC, ABG, 2D Echo |
| X-rays | Pelvis, thigh, right foot |
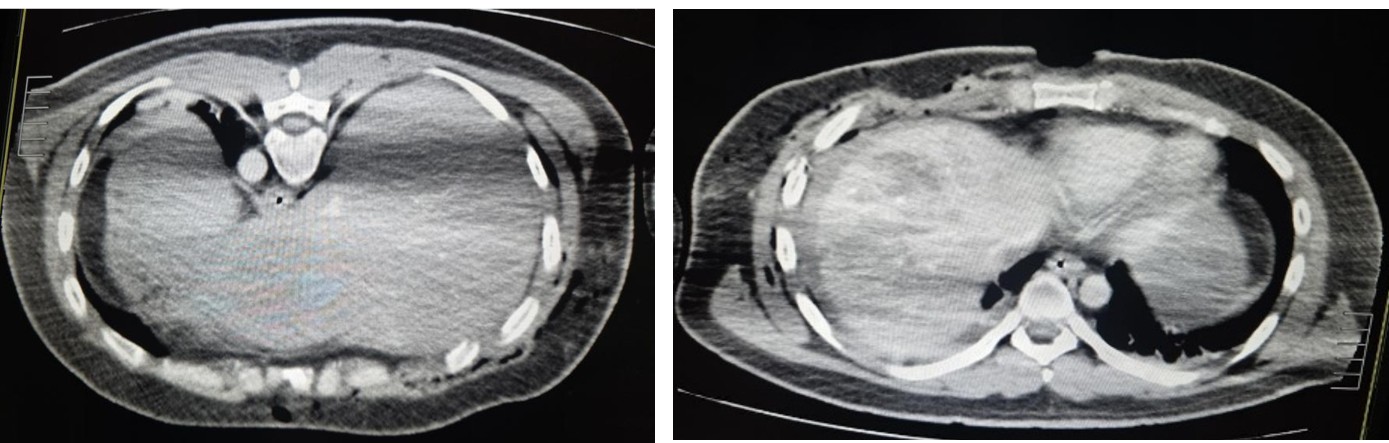
Fig (1): CT Abdomen
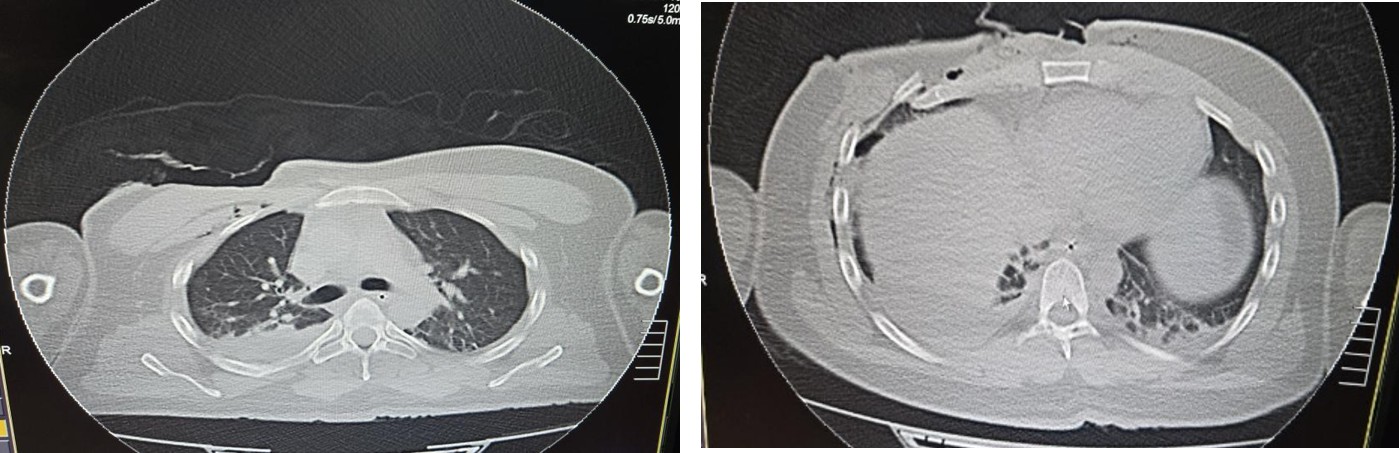
Fig (2): CT Chest
Diagnosis
- Blunt trauma to right chest and abdomen
- Multiple right-sided rib fractures
- Right chest wall muscle laceration
- Grade III liver injury
- Mild right kidney contusion
Management
Initial Management (Primary Survey – ABCDE)
- Airway: Intubated and airway secured
- Breathing: Oxygen therapy, ventilatory support
- Circulation: IV fluids, bleeding control
- Disability: Neurological monitoring
- Exposure: Full trauma assessment
Definitive Management
- Emergency exploration of right chest wound
- Surgical rib fixation of 5th, 6th, 7th ribs
- Flap closure of chest wall defect
- Wound debridement and muscle reconstruction
- Conservative management for liver laceration
- Urology consultation → conservative management of renal contusion
- Pain management: NSAIDs, opioids, intercostal nerve block
- Chest physiotherapy
- Oxygen support and respiratory care
- Sterile wound dressing and infection prevention
Post-Operative Course
Post-Operative Day (POD) 1
On the first postoperative day, the patient remained hemodynamically stable. He was awake, obeying verbal commands, and able to initiate spontaneous breaths with ventilator assistance. Oxygen saturation remained satisfactory under supportive ventilation. Adequate urine output indicated stable renal perfusion despite associated renal contusion.
Pain was controlled with multimodal analgesia, including intravenous opioids and intercostal nerve block support. Chest physiotherapy began in a modified form, focusing on gentle deep-breathing exercises to promote lung expansion while minimizing discomfort. Wound inspection showed healthy muscle reconstruction with no active bleeding.
Post-Operative Day (POD) 2
By the second postoperative day, the patient was afebrile and stable, with improving respiratory parameters. However, local examination of the chest wall surgical site revealed early signs of skin-edge necrosis, likely due to tissue handling and underlying crush injury. The necrotic changes remained localized, with no evidence of wound infection or purulent discharge. Intercostal drainage showed minimal serosanguinous output, and ventilator settings were gradually reduced as tolerated. Repeat laboratory investigations demonstrated stable haemoglobin and inflammatory markers within acceptable limits. Conservative management of liver and renal injuries continued, with no signs of hemodynamic deterioration.
Post-Operative Day (POD) 3
On the third postoperative day, the patient showed further clinical improvement. He was alert, fully oriented, and maintaining stable vital parameters. Respiratory status improved, with minimal intercostal drainage and satisfactory lung expansion on auscultation. Chest physiotherapy sessions were intensified to reduce the risk of atelectasis and optimize pulmonary recovery. The wound edges with necrosis were closely monitored for progression, and regular sterile dressings were continued. No systemic signs of infection were noted. Renal function remained stable with adequate urine output. Abdominal examination revealed no signs of worsening liver injury or internal bleeding. Gradual mobilization was initiated with assistance, and the patient tolerated sitting up and short-duration physiotherapy sessions.
Nursing Management
Airway and breathing
- Maintained airway patency by ensuring proper positioning of the endotracheal tube and monitoring for tube displacement, secretions, or obstruction.
- Monitored respiratory pattern, including depth, effort, use of accessory muscles, and rate to detect early signs of respiratory distress.
- Continuous pulse oximetry was used to assess oxygen saturation and evaluate the effectiveness of ventilatory support.
- Administered oxygen therapy as prescribed, adjusting oxygen delivery devices during weaning from mechanical ventilation.
- Positioned the patient in Semi-Fowler’s position, which improved lung expansion, reduced diaphragmatic pressure, and enhanced ventilation.
- Assisted with chest tube care by monitoring drainage amount and characteristics, maintaining chest tube patency, ensuring proper water-seal function, and observing for air leaks or signs of tube obstruction.
Pain management
- Assessed pain intensity regularly using a standardized pain scale.
- Administered prescribed analgesics, including opioids and NSAIDs, ensuring timely and adequate pain control.
- Monitored for side effects of analgesics, such as respiratory depression, hypotension, or sedation.
- Supported the chest with a pillow during coughing (splinting technique) to reduce pain during respiratory exercises.
- Reduced external stimuli and minimized painful procedures, ensuring coordinated care to avoid repeated discomfort.
Circulation and hemodynamic monitoring
- Frequently monitored vital signs, including BP, pulse, SpO₂, respiratory rate, and temperature, to detect hemodynamic instability.
- Observed for signs of shock, such as tachycardia, hypotension, cold extremities, diaphoresis, and altered mental status.
- Monitored urine output hourly, as an indicator of renal perfusion and ongoing blood loss.
- Assessed abdominal girth and tenderness to detect worsening internal bleeding.
- Supported intravenous fluid therapy and ensured patency of IV lines.
- Monitored laboratory values, including haemoglobin, haematocrit, electrolytes, and ABG results, to guide clinical management.
Wound and soft tissue care
- Assessed the wound for bleeding, swelling, discharge, or necrosis, particularly observing the compromised skin edges noted on POD-2.
- Performed sterile dressing changes according to surgical protocol to prevent infection and promote healing.
- Administered antibiotics as prescribed and monitored for signs of systemic infection such as fever, chills, or elevated WBC count.
- Assessed the surrounding skin for erythema, increased warmth, and signs of cellulitis or flap failure.
- Documented wound characteristics daily, including size, necrosis progression, and drainage amount.
Prevention of respiratory complications
- Monitored for signs of pneumothorax or haemothorax, such as sudden dyspnoea, cyanosis, decreased breath sounds, tracheal deviation, or increased chest tube drainage.
- Performed frequent auscultation to identify changes in breath sounds that might indicate fluid accumulation or lung collapse.
- Encouraged deep breathing exercises, early mobilization, and incentive spirometry to improve ventilation.
- Assisted the patient during mobilization, preventing fatigue and ensuring safety.
- Observed for productive cough, sputum colour, and respiratory secretions, reporting abnormalities promptly.
Gastrointestinal and renal monitoring
- Assessed abdominal pain, guarding, and distension for signs of worsening organ injury.
- Monitored bowel sounds and gastrointestinal function.
- Measured urine output; monitored colour for haematuria, indicating renal involvement.
- Ensured conservative management protocols (rest, hydration, monitoring) were followed.
Mobility and positioning
Encouraged early mobilization with assistance to prevent venous thromboembolism.
- Repositioned the patient every 2 hours to reduce pressure ulcers.
- Supported safe ambulation while monitoring pain and respiratory effort.
Psychosocial support and education
- Provided emotional reassurance to reduce anxiety related to trauma and surgery.
- Explained procedures and progress to enhance cooperation.
- Educated the patient on breathing exercises, wound care, and activity modifications for discharge.
Outcome
By the postoperative period, the patient showed steady clinical improvement. He remained alert, oriented, and hemodynamically stable with no signs of respiratory distress. Oxygen saturation was well maintained, and chest tube output was minimal without evidence of pneumothorax or haemothorax. Renal function and urine output remained adequate, supporting successful conservative management of the renal injury. The chest wall wound demonstrated healthy healing, with early necrosis remaining localized and non-progressive. Abdominal findings were stable, and the patient tolerated oral intake well. Overall, the patient showed marked improvement in respiratory function, wound healing, and pain control, indicating a favourable recovery.
Discharge
The patient was discharged after achieving stable clinical recovery following surgical and multidisciplinary management. At discharge, he was hemodynamically stable, afebrile, and maintaining adequate oxygen saturation on room air. Pain was well controlled, and respiratory effort had significantly improved. The chest wall wound showed healthy granulation with no signs of infection, and the intercostal drain had been removed after confirming satisfactory lung expansion. Abdominal and renal assessments remained stable, with adequate urine output and no signs of worsening organ injury. The patient was tolerating oral feeds, ambulating with assistance, and independent in basic activities. He and his family received education on wound care, breathing exercises, activity modification, and warning signs requiring immediate attention. Clear follow-up appointments with surgery, pulmonology, and urology were provided to support continued recovery at home.
Discussion – Medical Aspects
Blunt thoracic trauma poses significant risk due to potential respiratory compromise and rapid clinical deterioration. Multiple rib fractures impair chest expansion and ventilation, predisposing patients to hypoventilation, atelectasis, and pneumonia. Early imaging, particularly CT scan, is essential for identifying associated injuries such as lung contusion, liver laceration, and renal trauma. In this case, the Grade III liver injury and mild renal contusion were successfully managed conservatively because the patient remained hemodynamically stable. Conservative treatment is widely accepted for stable solid-organ injuries and reduces the need for unnecessary surgery. Surgical rib fixation played a key role in improving respiratory mechanics, providing pain relief, and enhancing postoperative pulmonary function. Timely wound exploration and flap closure were critical for managing the extensive chest wall laceration and preventing infection. Overall, early diagnosis, appropriate use of imaging, surgical stabilization of the chest wall, and conservative management of abdominal organ injuries contributed significantly to the patient’s favourable outcome.
Discussion – Nursing Aspects
Nursing care played a vital role in the recovery of this patient with blunt thoracoabdominal trauma. The primary focus was on maintaining airway patency, supporting adequate ventilation, and closely monitoring respiratory status, as multiple rib fractures significantly impair chest expansion and increase the risk of atelectasis and pneumonia. Effective pain management was essential, as uncontrolled pain can further limit breathing and mobility. Through timely analgesic administration and comfort measures such as chest splinting, nurses facilitated better respiratory effort and early mobilization. Wound management was another key component, especially due to the open chest wall injury and flap reconstruction. Regular assessment, sterile dressing care, and monitoring for signs of infection or necrosis helped promote healing and prevent complications. Continuous hemodynamic monitoring was critical given the associated liver and kidney injuries. Nurses played an important role in detecting early signs of internal bleeding or shock by observing vital signs and urine output. In addition to physical care, nurses provided education on breathing exercises, mobility, and wound care, and offered psychological support to reduce anxiety. Coordination with the multidisciplinary team ensured consistent, comprehensive care throughout the patient’s recovery.
Conclusion
This case underscores the critical importance of early diagnosis and a well-coordinated trauma management approach in patients with blunt thoracoabdominal injuries. Prompt imaging and accurate assessment allowed timely identification of multiple rib fractures, chest wall laceration, and associated abdominal organ injuries. The combination of appropriate surgical intervention particularly rib fixation and wound reconstruction and meticulous nursing care played a pivotal role in stabilizing the patient and supporting recovery. Continuous monitoring, effective pain management, and vigilant prevention of respiratory and wound-related complications further enhanced outcomes. Overall, this case demonstrates that a multidisciplinary, patient-centred approach is essential for minimizing morbidity and ensuring optimal recovery in complex trauma cases.
