Successful management of traumatic lung injury using Veno-venous ECMO in a young RTA patient
S. Pavithra1*, Mohammed Faizal2
1OT Staff Nurse, Kauvery Hospital , Tirunelveli, Tamil Nadu
2Anesthesia Technician, Kauvery Hospital, Tirunelveli, Tamil Nadu
*Correspondence
Case Presentation
Mr. XY is a 49-year-old male patient currently admitted to the Neuro ICU. Alleged H/O RTA (Road Traffic Accident) – 2-wheeler vs 4-wheeler on 17/02/2026 around 7:30 PM. Patients were initially treated at VMCH and later referred here for further management. Upon admission, the patient was intubated
GCS: 8/15
LOC: Present
Injuries noted
- Head injury
- Multiple rib fractures – Right side
- Right pneumothorax
- Right Femur Fracture
- Multiple lacerations over face
On Examination
| CVS | S1, S2 + |
|---|---|
| RS | Right AE ↓, Left AE +, Bilateral crept + |
| SpO₂ | 94% on MV support |
| CNS | Patient conscious, bilateral pupils 2 mm reacting to light. |
Initial Treatment Given
- Antifibrinolytics
- Antibiotics
- Antiepileptics
- Antiemetics
- Injection Perfalgan + Midazolam
- Other supportive drugs
Investigations: Blood investigations done, reports enclosed.
CT Report: Cutaneous laceration with air pockets in right frontal region.
HRCT Chest Report
- Fracture of 2nd, 5th, 6th ribs
- Undisplaced fracture of 3rd, 5th ribs
- Other imaging reports enclosed.
Specialty Reviews
- Neurosurgeon reviewed the patient.
- Opinions obtained from Ortho, Cardiothoracic surgeon,
- Pulmonology, Gastro, General surgeon.
ETU/ER Review: Advised Right ICD (Intercostal Drainage) insertion for pneumothorax.
Chief Complaints
The patient was admitted following an alleged road traffic accident involving a collision between a two-wheeler and a four-wheeler. The incident occurred at 7:30 PM on February 17, 2026, at the Ayyur road junction, resulting in a documented loss of consciousness.
Details of Present Illness
- Multiple rib fractures on right side
- Right pneumothorax
- Right Femur Fracture
- Patients got admitted in ICCU/ICU for further management
Associated Injuries
- Head injury
- Multiple lacerations over face
Past History
- No H/O fever, cold, seizures, vomiting
- No known diabetes or hypertension
- No alcohol / non-smoker
- History of Past Illness: Nil comorbid illness
Examination
| CVS | S1, S2 present |
| RS | Right AE ↓, Left AE +, Bilateral crepitations + |
Vitals
| SpO₂ | 100% with MV support |
| BP | 130/70 mmHg |
| HR | 121/min |
| RR | 16/min |
| Temp | Normal |
| CNS | Unconscious |
| Pupils | Bilateral 3 mm reacting |
Plan
ETT with mechanical ventilation (ETT + MV support) Provisional Diagnosis RTA – Poly trauma Right pneumothorax Multiple rib fractures (Right side) Focus ICD (Intercostal Drain) inserted Collection about 1.3 cm Lung expansion about 3 cm
- Right side pneumothorax
- Right pleural cavity filled with air
- CT – Trauma major package
- X-ray Chest – AP view
- X-ray Right Femur
- X-ray Right Shoulder
- X-ray Right Leg
Proposed Care Plan
- Intubation with MV support
- ICD insertion
- IV fluids
- NS infusions
Medications
- Xone 1 g IV BD
- Pan 40 mg IV BD
- Emeset 4 mg IV BD
- Tranexamic acid 1 g IV stat
Indication for ECMO
- Severe hypoxemia does not respond to mechanical ventilation
- Hemodynamic instability
- ARDS
ECMO team
Date : 22–23 Feb 2026
Team : Dr. Arun Singh / Dr. A.P.S. Kannan / Dr. Selvi
Patient Vitals
- BP: 100/90 mmHg (on Noradrenaline infusion)
- PR: 86/min
- SpO₂; 83%
- P/F ratio: <100 × >12 hrs
- Indicates severe hypoxemia
- Clinical Decision
- Attenders informed about need for ECMO
- Prone positioning not possible
Risks explained
- Increased bleeding
- Multiple transfusions
- Prolonged ICU stay
- Decision: Proceeded for VV-ECMO
ECHO Findings
- LV EF: 50%
- RA/RV: Normal
- TAPSE: 1.8 cm
- IVC: 1.2 cm, collapsing
- Suggests preserved cardiac function → suitable for VV ECMO
- Lung Ultrasound (USG)
- B/L B lines present
- Left > Right
- Indicates severe lung involvement (likely ARDS)
- ECMO Procedure Notes (23-02-2026 | 1:00 PM)
Preparation
ECMO procedure
- Patient evaluated and decision taken for ECMO cannulation under sterile precautions.
- Patients sedated and intubated.
- Monitoring lines secured.
- Cannulation done via femoral vein / internal jugular vein
- ECMO circuit connected.
- Adequate blood flow established.
- Oxygenation improved after initiation.
Medications
- Heparin infusion for anticoagulation
- Sedation and analgesia
- Antibiotics
- Inotropic support (if required)
- Monitoring Plan
- Continuous ECG monitoring
- ABG monitoring
- ACT / coagulation profile
- ECMO circuit monitoring
- Intake and output charting
Plan
- Continue ECMO support
- Daily assessment for weaning
- Monitor for complication
- Whole body draped
- TEE placed
Cannulation Details
Guidewire Placement (Right Femoral Vein)
- Micro puncture access
- 7 Fr sheath placed
- 150 cm guidewire placed
- Confirmed under TEE guidance
Serial Dilatation
Femoral vein: 12 Fr → 24 Fr → 26 Fr
Cannula Insertion
Femoral cannula: Mac Vic Multistage Venous Cannula 26 Fr inserted under TEE
Return cannula (IJV) inserted
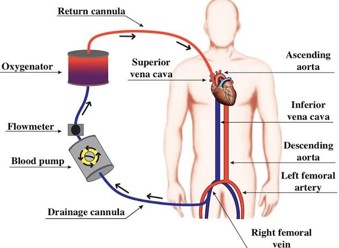
Image Source: Tarig Eltoum Fadelelmoula, researchgate, May 2020
Right IJV
- Micro puncture needle used
- 7 Fr sheath placed
IJV: MAQUET 17 FR ARTERIAL CANNULA
- Fixed at 15 cm
- Anticoagulation
- Heparin 5000 IU IV given
- ACT monitored
ECMO Initiation
- Flow established
- RPM gradually increased
- No chattering
ECMO Settings
- Mode: VV ECMO
- Blood flow: 4.2 L/min ~3500 RPM
- Sweep gas flow: 4 L/min
- FiO₂: 100 %
- Patient Status Post ECMO
- Hemodynamically stable
- Oxygen saturation improved
- Ventilator support continued
- Urine output monitored
Chest X-ray (AP View) – Interpretation
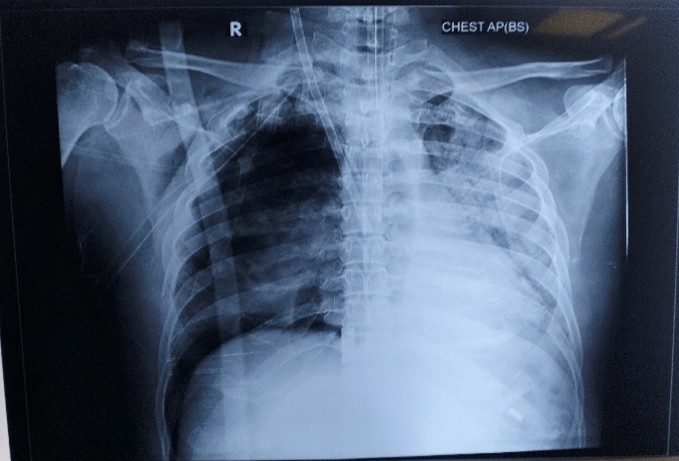
Technical
- View : AP (Bedside)
- Marker : Right (R) side visible
- Likely ICU patient (portable film)
Lines / Tubes
- A tube is seen in the trachea → likely endotracheal tube (ET tube)
- Position appears roughly within trachea, but exact tip level needs confirmation (ideal: 2–3 cm above carina)
Lung Findings
- Bilateral lung opacities present
- Left lung > Right lung involvement
- Patchy / diffuse white areas → suggest:
- Consolidation
- Pulmonary edema or ARDS pattern
This correlates with your earlier note of:
- Low SpO₂ (83%)
- Low P/F ratio (<100)
Right Lung
- Relatively more aerated (darker) compared to left
- Still shows patchy involvement
Left Lung
- Dense opacification (whiter)
- Suggests:
- Severe consolidation
- Fluid-filled alveoli
- Possibly dependent collapse or ARDS
- Cardiac Silhouette
- Appears slightly enlarged or obscured
Could be due to:
- AP view magnification
- Lung pathology masking borders
Pleura
- No obvious large pneumothorax
- Effusion not clearly defined (possible on left side but needs clinical correlation)
Chest X-ray (AP Bedside) – Interpretation
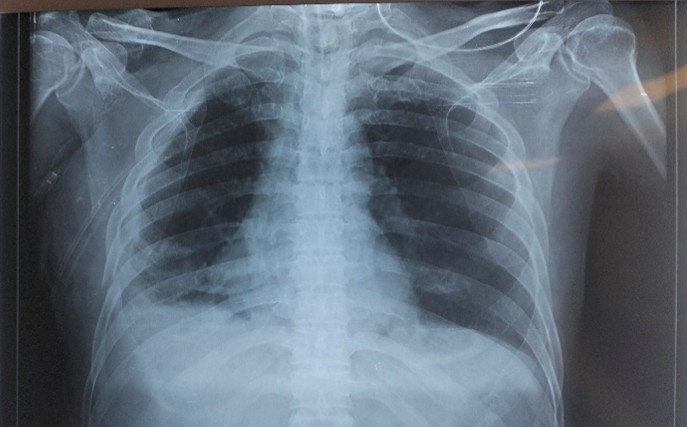
Date: 12-03-2026
View: AP bedside
Comparison Insight (vs previous X-ray)
- This film appears improved compared to earlier one:
- Less diffuse white-out
- Better lung aeration
- Lung Fields
- Bilateral lung expansion improved
Residual findings:
- Mild-to-moderate basal opacities
- More on the lower right zone
- Upper zones are relatively clearer
Suggests
- Resolving ARDS / pulmonary edema
- Residual basal consolidation or atelectasis
- Right Lung
- Patchy opacity in lower zone
Possible
- Atelectasis
- Residual consolidation
- Small pleural effusion
Left Lung
- Significantly cleared compared to prior
- Mild basal haziness persists
- Cardiac Silhouette
- Appears within normal limits (considering AP view)
- Pleura
- No obvious pneumothorax
- Possible minimal basal effusion (especially on the right side)
Devices / Lines
- No obvious ET tube seen in this film
- No clear ECMO cannula visible (may be removed or not in field)
Overall Impression
- Interval improvement
- Previously severe bilateral opacities → now partially resolved
Status likely
- Recovering ARDS
- Post ventilation / ECMO support improvement
Clinical Correlation
This X-ray suggests
- Improved oxygenation likely
- Weaning phase (ventilator/ECMO) possible
Continue monitoring for:
- Basal collapse
Decannulation notes
Patient successfully weaned and de-cannulated from ECMO with stable hemodynamics and adequate oxygenation, patient stable, cannulas removed, hemostasis achieved.
- No bleeding /hematoma
- SpO2 – 100% on ventilator.
Reference
- Pearson DT. Gas exchange: bubble and membrane oxygenators. Semin Thorac Cardiovasc Surg. 1990 Oct;2(4):313-9. [PubMed]
- Haworth WS. The development of the modern oxygenator. Ann Thorac Surg. 2003 Dec;76(6):S2216-9. [PubMed]
- Lafç G, Budak AB, Yener AÜ, Cicek OF. Use of extracorporeal membrane oxygenation in adults. Heart Lung Circ. 2014 Jan;23(1):10-23. [PubMed]
- Thompson BT, Chambers RC, Liu KD. Acute respiratory distress syndrome. N Engl J Med. 2017;377(6):562-572.doipubmed
- ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526-2533.doi
- Lepper PM, Barrett NA, Swol J, Lorusso R, Di Nardo M, Belliato M, Belohlavek J, et al. Perception of prolonged extracorporeal membrane oxygenation in Europe: an EuroELSO survey. Perfusion. 2020;35(1_suppl):81-85.doipubmed
- Ewig S, Hoffken G, Kern W, Rohde G, Flick H, Krause R, et al. Behandlung von Erwachsenen Patienten mit ambulant erworbener Pneumonie und Pravention – Update 2016. Pneumologie. 2016;70(3):151-200.doipubmed
Nightingale Journals
- Editorial
- Nursing care of patient with arrhythmia in various scenario at non critical and critical ward
- Arrhythmia Identification and Differentiation
- Pediatric arrhythmias diagnosis and management in children
- Understanding electrocardiography fundamentals and its interpretation
- Non-Pharmacological management of arrhythmias
- The science behind arrhythmias: Pathophysiology and causes
- A comprehensive review on ABG Analysis
- Airway Management: An overview
- Exploring different ways to deliver oxygen
- Management of raised ICP
- Paediatric early warning score: Good tool for clinical practice
- Enhancing continuity and safety in critical care: Through effective documentation and structured handover
- Implementation of evidence-based care bundles to prevent healthcare-associated infections
- Prevention and management of pressure injuries in clinical settings
- Safe transport of critically ill patients: Principles, protocols and best practices
- The vital role of nurses in critical care procedures: A focus on pre-procedure preparation
- Anatomy and Physiology of Kidney
- Anemia in Kidney Disease
- Fluid and Electrolyte Imbalance
- Hypertension and diabetes mellitus management in kidney disease
- ESRD: Palliative Care
- Care of Hemodialysis and peritoneal dialysis patients
- In house Continuing Nursing Education (CNE) on “Diabetic Foot Care” at Kauvery Hospital, Cantonment
- Patient Education on Foot Care Nursing Role
- In-House-Continuing Nursing Education (CNE) on “Basic Concepts of Nursing in Polytrauma” Kauvery Hospital, Tennur – 2025
- Assessment and Resuscitation of Head Injury
- Initial Assessment of Trauma Patients
- Monitoring and Prevention of complications During the Transfer of Polytrauma Patients
- Role of Critical Care Nursing in Polytrauma Management
- Anatomy and Physiology of Skin
- Diabetic Wound Care Management
- High Risk for Developing Pressure Injuries
- Medical Device Related Pressure Injury
- Prevention of Surgical Site Infections
- Wound care: An overview
- Wound Healing: An overview
- Editorial
- A case of hypoxic ischemic encephalopathy
- A case of multiple tablets overdose
- From elective surgery to mechanical ventilation: A critical post sterilization nursing care: A case report
- A rare case of Kikuchi disease with recurrent symptoms
- A journey from thrombolysis to decompressive craniectomy and lifesaving fasciotomy
- Arrhythmogenic right ventricular dysplasia presenting as ventricular tachycardia in an adolescent: A case report
- Deep right capsuloganglionic high-flow arteriovenous malformation presenting with intracerebral hemorrhage in an adolescent: A comprehensive case report
- Posterolateral thoracotomy for tumor excision
- Ventricular septal defect repair
- Cardiac myxoma and beyond: A case of benign tumor
- Learned Helplessness in Maternal Health: Implication for Maternal Well-being and the Transformative Role of Nurses
- Allergic Bronchopulmonary Aspergillosis (ABPA): The medical nutrition therapy for ABPA
- Handgrip dynamometry and anthropometric measurements for assessing nutritional repletion in malnourished cancer patients undergoing nutrition support
- Sudden cardiac arrest with super-refractory seizures in a patient with bilateral temporal lobe meningioma and end-stage renal disease
- Spectrum of supraventricular and ventricular arrhythmia’s: A case series highlighting AVNRT and arrhythmogenic right ventricular dysplasia
- The combination approach of rosuvastatin and ezetimibe in post-stent patients
- Hypoglycemic encephalopathy with diffuse cerebral edema and multi‑organ dysfunction: Perspective on a patient with type 2 diabetes mellitus
- Complicated UTI with MDR Pseudomonas in an elderly patient managed with combination antibiotics and DJ stenting
- Non-Obstructive Hypertrophic Cardiomyopathy presenting with asymptomatic: A Case Report
- Awake craniotomy for left frontal high-grade glioma: a multidisciplinary case report
- Journal Scan: A review of images in clinical medicine of immediate clinical significance, harvested from major international journals
- Editorial
- A case of Acute C5 – C6 Compressive myelopathy with bowel involvement
- A Case of Acute lymphoplastic leukemia
- A case of cerebellar hemangioblastoma causing obstructive hydrocephalus
- A case of thymoma
- Acute food-induced anaphylaxis in an elderly male with comorbidities
- A case study on congenital cyanotic heart disease with Ventricular Septal Defect (VSD) managed by surgical closure with RVOT resection
- Calcific AS and TAVI
- Conduction System Pacing (CSP)
- A case report on DCLD with hepatic encephalopathy and multidrug resistant sepsis
- Surgical management of necrotizing pneumonia with advanced empyema in a 3-year-old child: A case report
- Comprehensive approach to tuberculosis care: insights from a regional workshop at Kauvery hospital, Electronic city
- Hypokalaemia induced paralytic ileus
- Role of bubble contrast echocardiography in the diagnosis of hepatopulmonary syndrome
- Cerebral venous thrombosis with intracerebral hemorrhage in a patient with C1Q nephropathy and acute pancreatitis: a rare clinical constellation
- A retrospective study to assess postoperative pain levels among patients undergoing IPOM and E TEP hernia repair
- Bilateral uterine artery embolization
- Paraquat Poisoning
- From clinical examination to CT diagnosis: An emergency nurse–led approach to acute abdominal pain
- Unmasking hidden hypoxia: A case of methemoglobinemia in a young adult
- Emergency nursing management of massive upper GI bleed
- Successful management of severe sepsis with respiratory failure following live renal transplantation
- Acute Fatty Liver of Pregnancy
- Tracheoesophageal fistula repair
- Message from Dr. Manivannan Selvaraj, Founder and Managing Director, Kauvery Hospitals
- EDITORIAL
- Editorial Board
- Voices from the field!
- Junior nurses in Kauvery Hospital on the frontline against the COVID-19 pandemic
- Challenges in nursing care in achieving a successful outcome to a Liver Transplant on a 2-year old child with life threatening genetic condition
- Nursing management of a multi-organ transplant (Liver and Kidney) on an adolescent
- Successful discharge of a four year old baby with life threatening gas gangrene and compartment syndrome
- The revolutionary effect of a nursing-driven initiative to reduce ICU re-admissions
- Nephrotic syndrome: A case report
- Nursing Care of Patient with Thoracic Endo vascular Aortic Repair (TEVAR)
- Efficient Nursing Care equals Early Recovery
- Umbilical Cord Blood Banking is a lifesaver for your family, “Create one life, save another”: A review
- Challenges associated with wearing gloves
- Certificate Course on Infection Control 2022
- The ANEI Young Leader Award, 2022, comes to Kauvery Hospitals!
- The AHPI Nursing Excellence Award 2022, comes to Kauvery Hospital, Tennur
- Editorial
- Editorial Board
- Caring is the Essence of Nursing
- To be patient and calm! Why I Love Working as an Emergency Room Nurse
- Infective Endocarditis
- Infective Endocarditis
- Patent Ductus Arteriosus
- HOSPITalk 2023 – Clinical Governance
- Cardiac healthy diet
- Healthy diet for people working night shifts
- Chimeric antigen receptor (car) T cell therapy
- Human papillomavirus (HPV) vaccine
- Kauvery Hospital Journey on Winning National Level CII QC Competition Against the Industrial Sectors
- செவிலியர்கள் தின வாழ்த்து கவிதை
- அன்பு காவேரி
- Hepatology for nurses
- Role of Physiotherapy in Traumatic Brain Injury: A case report
- My experience at Kauvery Hospital, Salem
- Editorial
- Editorial Board
- Benign Paroxysmal Positional Vertigo (BPPV): A Case Series
- Nutrition for Nurses
- Cardiovascular effects of sodium – glucose co-transporter- 2 inhibitor, Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl-peptidase 4 inhibitors
- Brief Guide on Food Safety Standards to be Adopted Summer in South India
- Kauvery Hospital: Pioneering the Future of Healthcare with IoT, Wins Healthcare Asia Awards.
- மருத்துவர்கள் தின வாழ்த்து கவிதை
- காவேரியனின் தன்னம்பிக்கை
- வெற்றியின் பாதை
- Editorial
- Editorial Board
- A six-year-old girl gets a Permanent Pacemaker implanted!
- Cardio Renal Amyloidosis (Non-Secretory Myeloma)
- Deep Vein Thrombosis, treated with Angiojet Percutaneous Mechanical Thrombectomy (PMT): A Case Report
- Emergency CABG in Acute MI
- Meatotomy
- Septic Shock with Multiple Organ Dysfunction Syndrome: A Case Report
- Stab Injury: A Case Report
- The Journey of Dialysis Unit at Hosur
- The measure of life is not its duration but its donation
- Innovation at the frontline of Nursing: A Review
- A case study on hydatid cyst
- Untold History of British Scientist: Contributed to the Discovery of DNA
- Neurology for Nurses
- Poem
- மருத்துவாலயம்
- EDITORIAL
- Editorial Board
- Biological or circadian clock
- A novel direct thrombin inhibitor from tick salivary transcriptoms: A review
- Nursing Care of a Patient with Coarctation of aorta (COA)
- Nursing care of patient with aortic dissection
- Wireless moonlight: An ultra-short case study
- Acute liver failure: A case report
- We nurses hand-hold a patient on a long walk down a dark COVID road
- Effectiveness of segmental breathing and active cycle of breathing technique in the management of dyspnoea among covid-19 patients
- EDITORIAL
- Editorial Board
- I am a proud to be a Liver Transplant Nurse!
- Head Injury: A case report
- Postpartum/Peripartum Cardiomyopathy
- Nursing Care of Patient with Myocardial Infarction
- Nursing challenges faced in care of patient with Blunt Injury Abdomen
- Salicylate poisoning
- Vascular Access Management (VAM) training program for nurses
- Therapeutic Nutrition among Critical care patients
- Diagnostic Image: Palmar Hyperlinearity and Filaggrin Deficiency
- Journal Scan
- EDITORIAL
- Editorial Board
- Guideline-directed drug treatment for heart failure
- Dilated cardiomyopathy
- IV Proton Pump Inhibitors (PPIs): What are the true indications?
- Role of physiotherapy in GBS patients during hospitalization:A case presentation
- Pulmonary Thromboembolism
- Paraquat poisoning, an emerging problem, a challenging outcome
- Achievements of today are the stepping stones for success tomorrow!
- Diagnostic Image
- Chronic obstructive pulmonary disease: A case report
- EDITORIAL
- Editorial Board
- The Good Nurse
- Success story of a patient with Haemangioma
- Role of physiotherapy in Bell’s Palsy at outpatient department
- Arrhythmogenic Right Ventricular Dysplasia: A Cardiomyopathy
- Systemic Lupus Erythematosus (SLE)
- Teamwork makes a Dreamwork
- Cholecysto Cutabeous Fistula, an emerging problem: a challenging outcome
- Adhesive small bowel obstruction: Nutrition care process
- Diagnostic Image: Moderate Pitting Edema in Lower Limbs
- Editorial
- Editorial Board
- Quality improvement project to reduce the incidence of ventilator-associated pneumonia
- Rare disease, desired outcome
- Management of patients with acute myocardial infarction with ischemic stroke
- Left mediastinal tumor excision
- Esophageal varices grade III: A case report
- TB meningitis: A case report
- Nutrition care process for Sigmoid Diverticulitis
- Nutritional management of patient who underwent emergency laparotomy and GIST
- Nutritional management of gestational diabetes mellitus
- Nutrition and drug interaction
- மக்களின் நம்பிக்கை!
- காவேரித்தாய் – 2
- ஊசியின் மகத்துவம்
- Editorial
- Editorial Board
- Resilient and Empowered: The Unstoppable Force of Women’s Spirit
- “Global Perspectives on Patient Safety: A Recap of the International Patient Safety Conference – 13th to 14th Feb 2023”
- Acute Pancreatitis: the nutrition care process
- Role of diet in mitral valve replacement: A case presentation
- Our colleague’s SVT (Supra Ventricular Tachycardia)!
- Overview of Acute Respiratory Distress Syndrome
- To prevent the negative impact of Inj. Amphotericin among Mucormycosis patients
- Diagnostic Cases: Spontaneous Abortion and Gangrene
- Effective Adherence of Checklist through Digitalisation
- Nephrology for Nurses
- “உயிரைக்காக்கும் உயரியதானம்”
- மக்களின் நம்பிக்கை
- Nightingale Journal Editorial – April Issue Highlights
- Editorial Board
- SVT (Supra Ventricular Tachycardia)
- Tender loving care of patient with DVT after IVF (in vitro fertilization)
- ASD Surgical Closure
- Quality improvement project to reduce the risk of cross infection from wall mounted suction apparatus
- Quality Improvement Project on Crash Cart Management with numbered seal
- Log the Indian Millets
- Crystal your body by dint of seven Crystal Seeds!
- Role of Glucagon
- Educative Image: Department of Orthopaedics
- Nephrology for Nurses! – Part 2
- EDITORIAL
- Editorial Board
- இதயநகரத்தின் செவிலியர்கள் தின வாழ்த்து
- My experience as a patient
- A study on Anidulafungin therapy in oncology patients in a tertiary care hospitals
- A case study on Heart Transplantation
- Your Physiotherapist’s talks! Know your Moves
- Impact of air pollution on human health
- 4th QOK Group Level Competition 2023
- 7th International conference of CAHO
- செவிலியர் எனும் தாய்
- HEPATOLOGY FOR NURSES
- Editorial
- Editorial Board
- Unknown etiology, thoughtful management, gratifying outcomes!
- Antiphospholipid Syndrome(APLS) in a man
- World Organ Donation Day Celebration at Kauvery Hospital, Hosur
- Approach to cardiac arrest
- Cardiac Tissue Viability Study
- Dietary management after Mitral Valve Replacement
- Clipping of a Cerebral Aneurysm at Nellai
- Care of Chronic Suppurative Otitis Media (CSOM)
- Pituitary Macroadenoma: A case report
- Superior mesenteric artery thrombosis
- Pharmacists: The Silent Heroes of the Health Care System
- Educative Image
- Poem
- A battle to win a baby
- 5S Sustenance Level-Up for Salem, Hosur and ECB Units
- Editorial
- Prevention of accidental removal of tube and drains: A case report
- Clinical Report Workshop: An initiative by the Clinical Governance Team
- Burr Hole – evacuation of right frontoparietal chronic Sub Dural Hematoma and left parietal SDH
- Balloon Mitral Valvotomy
- Intra Pulmonary Thrombolysis
- Nephrotic Syndrome: A case report
- Trans catheter Aortic Valve Implantation (TAVI)
- Tetralogy of Fallot (TOF): Echocardiography
- Patent Ductus Arteriosus (PDA)
- A souvenir to remember the Nurses day 2024: Celebration of the Guardian angel of Healthcare
- Flying Cherub
- காவேரியின் செவிலியராய்!
- காவேரியின் பசுமை புரட்சி
- Editorial
- Care of patient with Interstitial Lung Disease
- Ovarian Torsion: A case report and discussion
- Ovarian torsion: A case report
- Acute Respiratory Distress Syndrome: A case report
- Shadow reports of heart city’s valve diseases and clinic
- Innovative strategy, empowerment and amendment of guidelines to prevent IV complications
- Effectiveness of Nurse- fabricated innovative device (K-Brace) on prevention of phlebitis
- Organ Donor Hero!
- Understanding Thalassemia: A comprehensive overview
- Pressure Injuries—the sensitive indicator
- The sixth QOK Competition April 2024
- Editorial
- Infective Endocarditis (IE)
- A case report on Bull Gore Injury
- Free Flap for traumatic raw area: A case report
- The Story of the “First Cry”
- Case series on drug-induced anaphylactic shock
- Clinical therapeutics: The adrenergic system and related drugs
- Flying angel experience
- From QOK to KOACH: A journey of continuous improvement
- Poem – காவேரியின் நவீன ஐந்து எஸ்(5S) மாடல்
- Editorial
- Editorial Board
- Attempted Hanging: A case series
- Sub Arachnoid Hemorrhage due to Cerebral Aneurysm
- Acute Pulmonary Thromboembolism with Systemic Lupus Erythematous
- Down Syndrome with Severe Pulmonary Stenosis
- Bentalls Procedure
- Glycogen Storage Disease (GSD)
- Nursing Care of Patient with Penetrating Chest Injury (Left Chest Wall)
- A child with Acute Inflammatory Demyelinating Polyradiculoneuropathy (AIDP) – Guillian- Barre Syndrome (GBS)
- Periampulatory carcinoma (Whipple’s procedure)
- Assisted delivery with Forceps Extraction
- Thrilling Moment on a Successful transportation of the cadaver donor liver to its recipient
- Editorial
- Transcatheter Aortic Valve Implantation (TAVI)
- Cautery Burns: A Clinical Audit
- Automatic Implantable Cardioverter Defibrillator (AICD)
- Thymectomy
- Deep Vein Thrombosis: A case report
- Mesentric Neoplasm
- QT Syndrome
- Healthy diet, affordable for all – Fuel for the Future
- Personalizing 5-FU Treatment in Head and Neck Cancer: A TDM Pilot Study
- Rapid Review of CNE -Nursing Challenges in Coronary Artery Diseases
- Preconference Workshop on International patient safety Goals (IPSG)
- Editorial
- Cerebral malaria: Management with artesunate
- Hypertrophic cardiomyopathy: A case report
- Incredible challenges and outcomes: A case report
- Prevention of extravasation in Oncology unit
- Management of germ cell tumors: A review
- Monocytes: The mysterious cell on the CBC
- Efficacy of individualized use of a multisensory integrative environment on engagement: In children with sensory modulation disorder
- Dietary guidelines and food safety: For immuno-suppressed/compromised patients
- Nutritional management: For a patient with triple vessel disease
- இயன்முறை மருத்துவமும் மறுவாழ்வும்
- உயிர் காக்கும் தானம்
- மாற்றத்தை விதைக்கும் திறனாளிகள்
- EDITORIAL
- EDITORIAL BOARD
- CEREBRAL MALARIA: A CASE REPORT
- CEFEPIME – TAZOBACTUM – INDUCED FLUID – FILLED BLISTERS (BULLOUS LESIONS): A CASE REPORT
- BLOOD TRANSFUSION REACTIONS: AN OVERVIEW
- EFFECTIVENESS OF REHABILITATIVE APPROACH-BASED MANAGEMENT FOR CHILDREN WITH JAPANESE ENCEPHALITIS (JE)
- THE EFFECT OF NUTRITIONAL COMPOSITION ON THE GLYCEMIC INDEX AND GLYCEMIC LOAD VALUES
- KCHS PRATIDHI RISES TO THE CHALLENGE: A TRIUMPH AT THE NATIONAL QC CONVENTION
- JOURNAL SCAN FOR THE CLINICAL PHARMACIST
- காவேரித்தாய் – 4
- EDITORIAL
- INSTRUCTIONS TO AUTHORS
- AORTIC ANEURYSM WITH PARAVERTEBRAL COLLECTION
- DEEP VEIN THROMBOSIS AT RIGHT UPPER LIMB: A CASE REPORT
- ENTEROVIRUS ASSOCIATED MENINGOENCEPHALITIS: A CASE REPORT
- CONGENITAL HEART DISEASE (ASD – OS): A CASE REPORT
- FUNCTIONAL SHORT GUT SYNDROME: A CASE CAPSULE
- PERI-OPERATIVE CARE DURING CYTOREDUCTION SURGERY (CRS) WITH HYPERTHERMIC INTRAPERITONEAL CHEMOTHERAPY (HIPEC): KAUVERY EXPERIENCE.
- A CASE REPORT: MYELOPROLIFERATIVE NEOPLASMS (MPNS) WITH CABG
- OVERVIEW OF BREAST FEEDING: A REVIEW
- PITUITARY MACRO ADENOMA-TRANS-NASAL TRANS-SPHENOIDAL ENDOSCOPIC EXCISION
- JOURNAL SCAN: A CASE REVIEW OF IMMEDIATE CLINICAL SIGNIFICANCE, HARVESTED FROM MAJOR INTERNATIONAL JOURNAL
- தயக்கம் தவிர்
- Editorial
- Editorial Board
- Case Report: A success story of IVUS: In a PTCA
- Case Report on Ovarian Torsion
- Nursing care for a child with Thrombophlebitis
- Drug Induced Hypersensitivity to Salazopyrin: A case report
- The Phytonutrients — 365.25 Days/52 Weeks of Phytonutrients help’s to develop our shape
- Role of diet in coronary artery disease
- 5S Cross Unit Assessment 2024
- என்னுள் 5S
- பெண்ணே பெருமை கொள்
- Journal scan
- Editorial
- Instructions for Authors
- Ventricular Septal Defect (VSD): Echocardiography
- Steven Johnson Syndrome: A case report
- A case review on Capsule Endoscopy
- Savoir Faire: A management for mass causality
- Case report on Gouty Arthritis
- Management of a road traffic accident victim with severe head injury, and aspiration: A case report
- A case report on inhalation of chlorine gas
- ST segment elevation during Treadmill exercise test in a patient without prior Myocardial Infarction
- History and evolution of Corporate and Clinical governance
- The need of Human Papilloma Virus (HPV) vaccine: A review
- Futuristic face of resuscitative Centhaquine for hypovolemic shock: A Review
- Boost your health in this summer
- A data-driven approach to patient care: Kauvery Hospital pioneers six sigma in healthcare
- Fascinating experience as a flying angel
- விளையாட்டுத் திடல்
- எங்கள் காவேரி
- Editorial
- Triple Bypass: A case report
- Boerhaave Syndrome with Mediastinitis
- Right sided Infective Endocarditis
- Marburg virus disease: A systematic review
- Advances in cardiac amyloidosis treatment: A review on Tafamidis
- Role of salt in human health
- Learning by playing: 5S makes school a breeze
- நம் காவேரி
- செவிலிய தேவதைகள்
- Editorial
- A case report: Melioidosis
- Type IV-A Choledochal cyst
- Nursing care of the patient with right lower lung foreign body and Bronchiectasis: Treated surgically with lobectomy
- Care of patient with OPC poisoning
- The Rosai-Dorfman disease presents with extranodal involvement and diagnostic challenges
- Open stab injury by a Bull
- In-house Continuing Nursing Education (CNE) on mastering the complexities of critical illnesses at Kauvery Hospital, Tennur, 2024
- Effectiveness of trigger point release and ultrasound therapy on Trapezitis
- Kauvery Hospital Trichy region’s journey towards 5S model hospital recognition
- A Triumphant journey to 5S sustenance level I
- Poem – இரத்த தானம்
- Poem – ஆசிரியர் தின நல்வாழ்த்துக்கள்
- Poem – ஆசையான ஆசான்
- Poem – அவள் ஓர் அறிவியல்
- Editorial
- A Case of Burns
- A Case of Diabetic ketoacidosis
- A Case of Osteoarthritis
- A Case of Stroke
- A Case of Acute Myeloid Leukemia
- Case Study on Blunt Injury induced AKI
- Integration of Recent Technology in the Operation Theatre Enhancing Patient Outcomes
- Nursing Care of Patient with Congenital Acyanotic Heart Disease for Diagnostic Cardiac Catheterization Done
- May Thurner Syndrome Vascular Condition of Postpartum
- Myocardial Infarction in a Young Patient
- Nursing Care of Patient with Dextrocardia
- Case Study on Left Gangliocapsular Intracranial Hemorrhage with Cranioplasty
- Silent Leaks, Loud Alarms: Nursing Vigilance in a Complex Neurosurgical Recovery
- From Crisis to Care: The Challenge of Managing Myasthenia Gravis in an Elderly Patient with Multiple Comorbidities
- Dual Intervention Success: Managing Bradycardia and Heart Failure with TPI and CRT – D
- A Case Report On Mastitis
- Our Nurses-Our Future: Investing in Nurses Empowerment for Enhancing the Nursing Workforce
- Empowering Patients in Patient Care – Prevention of Medication Error
- Case Publication Report: Malignant Ascites and Pleural Effusion in Stage 4 Ovarian Carcinoma – An Elaborated Case
- Case Study: Management of Thoracic Endovascular Aneurysm Repair (TEVAR) in an 82-Year-Old Male with Type B Aortic Dissection
- Case Study: A Rare Presentation of Type A Wellens Syndrome in a 45-Year-Old Male with Type 2 Diabetes Mellitus and Systemic Hypertension.
- A case report on Endometriosis
- Molar Pregnancy: A case report
- Review article of immune checkpoint inhibitors in cancer patients
- Case Study: Management of Kawasaki Disease in a Pediatric Patient
- Empowering Nurses through Hands-on BLS Training: A Large-Scale RNRM CNE Renewal Initiative by Kauvery Hospital, Trichy
- Editorial
- Empowering Clinical Participation Nurses Through Academic and Research participation
- From policy to practice: Transforming nurse competence through a restraint management recall program
- Peritoneal equilibration test in our CAPD patients: A retrospective analysis
- Perinatal asphyxia with hypoxic-ischemic encephalopathy stage I in a late preterm neonate: A case report
- A case of vibrio cholera
- Emergency nursing management of a patient with acute aortic intramural hematoma
- Case report on testicular cancer
- Case study on abdominal tuberculosis
- Monoclonal IgG kappa (IgGk) associated crescentic glomerulonephritis: A case of PGNMID in disguise
- Critical management of upper gastrointestinal bleed with septic shock in an elderly patient
- My experience in a renal transplant ICU
- Pulmonary vein stenosis
- A case report: Rheumatic heart disease and congestive heart failure in antenatal mother
- Case of corrosive poisoning with pneumonia
- A case report on Stevens Johnson Syndrome
- A case report on Sub Arachnoid Hemorrhage (SAH)
- Autosomal Recessive Polycystic Kidney (ARPKD) with cavernous transformation of portal vein
- A case report on open heart valve replacement
- Editorial
- The impact of home-based physiotherapy on functional capacity and quality of life in patients with severe heart failure
- Liver transplantation
- The Invisible Man – Androgen Insensitivity Syndrome: Disorders of sexual development
- Pericardial effusion
- A case report and discussion: Burns
- Challenges of polypharmacy in a geriatric patient with neurological disorder
- A case report on Bullous Pemphigoid (BP)
- Herpes Zoster Encephalitis: Diagnostic and Clinical Insights
- A Case Report & Review on Sternal Osteomyelitis
- Continuing Nursing Education on Prevention of Hospital Acquired Pressure Injury
- Prevention of Hematoma and Thrombus After CAG /PTCA
- Case Report: Neonatal Hirschsprung Disease
- Current Treatment, Challenges, and Research Updates in Sexually Transmitted Infections: A Detailed Review
- Lipoinjection for fat deficiency in right cheek
- LA Myxoma
- Nursing care of Sturge – Weber Syndrome (SWS), referred for Digital Subtraction Angiography (DSA)
- Nursing care of patient with Sick Sinus Syndrome
- Post-Partum Acute Kidney Injury
- Service Uniqueness and Management Outcomes (SUMO) in Healthcare Services
- Poem – அம்மா!!!
- Editorial
- When Banding Breaks, New Paths Awaken: The BRTO Revelation
- Smile Therapy
- Multidisciplinary approach to Thermal Burns
- Deep Brain Stimulation for Parkinson’s disease: A case report
- Zieve’s Syndrome: A review
- Acute Pulmonary Thromboembolism
- MPI scan guided revascularization in acute anterior wall Myocardial Infarction
- Ketogenic diet for Epilepsy: A case report and review
- Dietary management: Carcinoma in left buccal mucosa
- Malignant Middle Cerebral Artery (MCA) infarct and surgical decompression: Pre-op and post-op CT brain findings
- Cleistanthus collinus (Oduvanthalai poisoning): A case report
- My Experience as a Flying Angel
- In-house Continuing Nursing Education (CNE) on “Rapid Response Mastery
- Kauvery Hospital Salem’s Journey of 1st Ever Model Hospital
- மனமும் வெற்றியின் ரகசியமும்
- Editorial
- Against all odds: A road accident survivor’s journey to healing at Kauvery Hospital
- Clinical Case Report: Managing Hansen’s Disease in a 20-Years young girl
- Bilateral Internal Thoracic Artery Grafting for CABG
- Intra Pulmonary Thrombolysis
- A Case Report on Methotrexate-Induced Pancytopenia
- An Adult with an Atrial Septal Defect Presenting with a Brain Abscess
- Typhoid, a Prospective Observational Study
- Vancomycin – Therapeutic Drug Monitoring
- Cardiac’s Myxoma
- Mitral valve replacement
- Harmful effects of preservatives (Class 1) on Food Items
- In house Continuing Nursing Education (CNE) on “Shaping Excellence in Critical Care Nursing.” At Kauvery hospital, Cantonment.
- Poem – செவிலியர்
- Poem – ஒருபோதும் கேட்காதீர்கள்: “உனக்கு என்ன வேண்டும் என்று”
- Editorial
- A case report on Carbuncle
- Reverse Shoulder Arthroplasty: A case report
- A case report on severe dental caries with advanced lesions
- Supra ventricular Tachycardia: A case report
- A case of pernicious anaemia due to vitamin B12 deficiency
- A Journey of Miracles: Life Beyond the Deadly Trials for My Father
- A Victory day for CNE
- A Sapient Voyage – QCFI
- Tracheostomy: An overview
- முன்கூட்டியே கண்டறிவோம் புற்றுநோயை
- Editorial
- Emergency CABG for young female patient with critical coronary artery disease
- Meningomyelocoele: A case report and discussion
- Case study on Multiple Cranial Nerve Palsy and Necrotizing Pneumonia: The physiotherapy management
- Role of Physiotherapy in ACL Rehabilitation: A case report
- ASD Device Closure: Case report and discussion
- In-House-Continuing Nursing Education (CNE) on “Effective Nursing Strategies for Renal Transplantation” at Kauvery Hospital, Tennur
- காவேரியின் வாக்ஹோலிக் நடைபயிற்சி
- புத்தாண்டு
- Editorial
- Artificial Intelligence in Nursing: Enhancing Care and Reducing Burnout
- Report on comprehensive wound care workshop—elevating nursing excellence at Kauvery Hospital
- Cerebellopontine angle tumor
- Patient acuity score: Staffing plan
- Acute Respiratory Distress Syndrome
- Coronary Artery Disease and Carotid Stenosis: A dual threat
- Early-onset diabetic foot ulcers in CKD
- Nursing case study report: Reconstructive surgery for congenital TMJ ankylosis
- Care of severe ARDS and H1N1 Positive
- Whipple Procedure: A case report
- A milestone to remember in my career
- Poem – காதல்
- Poem – ஆரோக்கிய வாழ்வு – 2
- Editorial
- Management of Myelodysplastic Syndrome (MDS) with Probable Fungal Pneumonia
- Thrombotic Microangiopathy and Renal Cortical Necrosis in a Postpartum Patient: A rare and complex presentation
- Rising Star in Health care
- Systemic Lupus Erythematosus: A case report and discussion
- Effectiveness of Cardiopulmonary Resuscitation( CPR) and its Outcome
- Guillain-Barre syndrome
- Radiation-free ERCP in pregnancy
- Utilization of injection Sovateltide for acute ischemic stroke
- A case of severe malaria complicated by concurrent H 3 N 2 influenza infection: Diagnostic and therapeutic challenges
- Pulmonary Function Test Concepts
- Rapid Review of CNE – Enhancing Nursing Practice in Arrhythmia Management: Evidence Based Strategies
- நூறைக் கடந்த காவேரியின் மருத்துவ இதழ்(ஜர்னல்)
- பெண் என்பவள்
- வியக்கத்தகும் அதிசயமே! கண்டு வியக்கிறேன்
- Editorial
- Early Rescue PCI in Failed Thrombolysis in STEMI
- Internal Jugular Vein Thrombosis: A Case Report and Discussion
- The Beat of Compassion: A Clinical Presentation of Nursing Excellence
- Acute Necrotizing Pancreatitis: Challenges in Management and Recovery
- “From Struggle to Breathe to Freedom to Live”: The Miracle of Pulmonary Thromboendarterectomy
- Waugh Syndrome (Ileocolic Intussusception +Malrotation): A Case Report and Discussion
- Corrosive Poisoning: A Case Report
- Multiple Intracranial Aneurysms: A Case Report and Discussion
- Steroid-Dependent Nephrotic Syndrome in Pediatric Patients: Pharmacologic and Preventive Management
- Shared Decision-Making should be an Integral Part of Physiotherapy Practice: A Case Study on Total Knee Replacement
- NICU Graduate Day: “Saving the Unsavable” by Trusted Quality Care
- Balancing Technology and Patient Safety: Insights from the Workshop
- Impact of Nurse Leadership on Patient Outcomes
- பெற்றெடுக்காத அன்னை
- மனம் – ஒரு மாயை!
- Editorial
- Idiopathic Parkinson’s Disease
- A case report on Guillain–Barré Syndrome
- A case of Iatrogenic Mediastinitis
- A case of puerperal sepsis due to ESBL E. coli with multi-organ involvement: A clinical challenge
- Critical management of severe obstructive cholangitis with septic shock in an elderly patient with cardiac and renal comorbidities
- Acute cholecystitis after cardiovascular surgery (CABG)
- Comprehensive management of diabetic cellulitis in hand and its outcome
- A case of successful kidney transplantation after a long-term maintenance in haemodialysis
- “Mystery of Blue boy” Methemoglobinemia poisoning: Challenging in identification and treatment
- A case report on ovarian cyst torsion: Emergency procedure
- A case report on status epilepticus
- A new lease on life: Successful discharge after brain tumor
- The road to recovery: A case study on liver transplant success
- Systemic Lupus Erythematosus: A case report and discussion
- Carpal tunnel release surgery: A nursing case study on post-operative care
- Evidence-based nursing practice: A case study on Zadek’s procedure for ingrown toenail”
- Against the Odds: Impella-supported revival in an octogenarian with cardiogenic shock (stage E) and advanced coronary artery disease
- A structured approach for patient safety and experience: Enhancing traditional nursing practices with new dimension
- Nursing care of patient with penetrating left chest pain
- Through the crack of a blast, light of care found its way—Multisite Blast injury in a Farmer from Improvised Explosive Device: A Nursing Perspective
- Pulmonary Tuberculosis: A case study and clinical perspectives
- Secondary Postpartum Hemorrhage
- Care of patient with spondylodiscitis
- Nursing care of patient with cauda equina syndrome
- Editorial
- A case of spinal tuberculosis with acute spastic paraplegia managed with medical therapy and surgical fixation: A comprehensive clinical and nursing perspective
- Antiphospholipid antibody syndrome presenting as pulmonary thromboembolism and diffuse alveolar hemorrhage in a young female
- Ethical and clinical management of a jehovah’s witness patient undergoing deceased donor renal transplantation
- Effective management of type II endoleak post EVAR: A multidisciplinary approach by nurses
- Case Study: “Successful TAVI procedure for severe aortic stenosis, a patient’s journey”
- CRRT: More than renal replacement, a case study in multiple organ support
- Clinical practice guidelines on peripheral IV therapy practices
- Gulliain Barre Syndrome: A case report
- Case Report: Multiple sclerosis in a 28-year-young female
- Comparative case study report: Paraquat poisoning with multiorgan dysfunction
- Naegleria fowleri (Brain-Eating Amoeba): A comparative epidemiological and pathophysiological review—Global, Indian, and Kerala perspectives (2025)
- Patient safety colloquium 2025: “Safe care for every patient, every time”
- A lifesaving miracle: Bone marrow transplant gives six-month old baby a new lease of life
- The Healing of broken wings: A case of paediatric firecracker injuries
- Ureterovaginal Fistula Following Hysterectomy – A Clinical and Nursing Management Case Report
- Case Study: Adult-Onset Henoch–Schönlein Purpura (HSP)
- Desidustat: Role in management of anemia of chronic kidney disease (CKD)
- Comprehensive clinical management of an extensive lumbo-sacral wound with multiple sinuses in an elderly male
- Autoimmune encephalitis with anti-LGI1-antibody: A case report
- Case presentation on Total Knee Replacement
- In-House-Continuing Nursing Education (CNE): “Nursing Perspectives in Oncology”, Kauvery Hospital, Tennur
- Editorial
- Abdominal aortic aneurysm repair
- A case of ovarian cyst with partial torsion in an adolescent girl
- Clinical presentation and nursing care of a patient with acute ischemic stroke
- Nursing care of young patient with aortic valve replacement for bicuspid aortic valve and aortic valve stenosis
- Young patient care of abdominal aortic aneurysm repair
- Nursing management of multiple diagnoses and thrombectomy procedure
- Bypass to the future: A CABG success story
- A case report on pharyngeal fistula
- Chandipura virus: an overview
- Nursing case study: Management of right Common Iliac Artery (CIA) stenosis with Chronic Total Occlusion (CTO)
- Case study on peripheral arterial disease and its complications: Chronic limb threatening ischemia
- Foreign body removal: A case report
- The role of breast milk in enhancing nutritional and immunological properties
- A case report on sub dural hematoma in a patient on dual antiplatelet therapy
- Highly concentration electrolytes: A silent risk every nurse must recognize
- Transverse limb defect: A case report
- A quick review on the management of myasthenia gravis during pregnancy
- Youngest pediatric bone marrow transplant: Thalassemia major donor—thalassemia major marked sibling, bone marrow transplantation
- MOG antibody-associated optic neuritis: A case report
- Stuttering cerebrovascular accident and a rare intervention: A case report
- Thoracotomy with pleuropericardial window
- Enhancing healthcare leadership and sustainable team building through the OODA loop: insights from Kauvery hospital
- Clinical spectrum and management outcomes of GDM and GHTN: A case series from a tertiary care center
- The future of insulin: Innovations, AI, and the evolving role of pharmacists in diabetes care
- Editorial
- A bond beyond words—a beautiful truth when one twin can be the sibling’s life saver
- Acute limb ischemia in a young female with systemic lupus erythematosus
- A case report on laparoscopic retrieval of a massive gastric trichobezoar causing partial gastric outlet obstruction in a paediatric patient
- A complex neonatal presentation requiring Ladd’s procedure: A case report
- Effect of diet and lifestyle modifications on non-pharmacological HbA1c reduction in a new onset diabetes pre-renal transplant donors
- Pioneering the future: The first step in robotic surgery
- Neuromyelitis Optica
- Sleeve gastrectomy
- Multidisciplinary nursing approach to D6 vertebral collapse secondary to multiple myeloma
- Probable hereditary haemolytic anaemia with multisystem complications: A one-month clinical journey
- Type B Thoracoabdominal Aortic Dissection (TBAD) with fusiform aneurysm of infra-renal abdominal aorta
- Acute viral hepatitis
- Functional outcome of MOD QUAD procedure in a child with right sided Erb’s Palsy (Right Upper Limb)
- Paediatric hemangiomas of right lower eyelid excision: A case study from a nursing perspective
- Nutriotic table
- RTA with polytrauma injury
- Nutrition week celebration at Maa Kauvery Hospital
- Continuing nursing education on nurse’s role in infection prevention and control, in critical care unit
- Two type data analysis: Qualitative data vs Quantitative data
- Journal scan
- Editorial
- Dual kidney transplantation: An Emerging Strategy to Expand the Donor Pool
- A case of critical management of ILD
- A case of bilateral Congenital Talipes Equinovarus (CTEV)
- A case of gastric volvulus
- Penetrating stab injury to the neck (Zone II) with left subclavian artery injury and massive haemothorax
- Workshop on clinical audit and quality improvement projects: Strengthening nursing practice
- A case report on surgical retrieval of fragmented intravenous cannula tip from the cephalic vein
- The left sided mystery: Situs inversus totalis
- A challenging case of prolonged fever with acute kidney injury and multifocal neurological involvement
- Neglected right testicular tumor presenting as metastatic pleural empyema
- Successful pregnancy outcome in a primigravida with sick sinus syndrome on permanent pacemaker and previous cerebrovascular accident
- Exclusion of infra renal abdominal aneurysm with aorta bi-iliac bypass
- Cerebral fat embolism in a young polytrauma patient: A case report
- Dual surgical intervention in cardiac disease: A case study on CABG with AVR
- Successful management of refractory supraventricular tachycardia in a 4-month-old infant
- First successful neonatal percutaneous cardiac intervention done in Maa Kauvery & Heart city, Trichy
- Neuro Nursing – Quality Markers
- Drug of the month: Nitric oxide & nitrous oxide– Same family, different stories
- Multiple tablet overdose with multi-organ involvement and critical illness neuropathy: A case report from Kauvery Hospital, Trichy
- Amyotrophic Lateral Sclerosis (ALS): A case report
- Weight management for cancer patients
- Journal Scan
- Editorial
- A new milestone in spine care: spine endoscopy experience at kauvery hospital, trichy (Cantonment) – 2025
- Ethylene Glycol Poisoning Using Ethanol Therapy
- Robotic total knee replacement: First of its kind experience at Kauvery hospital, cantonment, Trichy – 2025
- Enhancing the safety of hospitalization by reducing patient falls
- Alcohol septal ablation for severe hypertrophic obstructive cardiomyopathy during pregnancy: Rare presentation
- C6 vertebral fracture secondary to tuberculous spondylodiscitis in a patient with chronic kidney disease
- Idiopathic intracranial hypertension presenting as recurrent cerebrospinal fluid rhinorrhea
- Critical pertussis
- Thinner Ingestion (Hydrocarbon Poisoning)
- Anaesthetic management of Oberlin Nerve Transfer without NMN-Depolarising muscle relaxants
- Tb meningitis–associated CNS vasculitis and stroke in HIV and diabetes: Highlighting multidisciplinary management
- From passive to active: Clinical reasoning in acute care chest physiotherapy
- Revision detethering surgery in a child with tethered cord syndrome associated with split cord malformation type II
- Thymoma (Anterior Mediastinal Mass)
- Laparoscopic bilateral etep mesh repair of bilateral recurrent right giant inguinoscrotal hernia + resection anastomosis of small intestine
- Management of post-renal biopsy pseudoaneurysm and rapidly progressive renal failure in a patient with IgA nephropathy
- Poly trauma patient care: A nursing approach
- Lenacapavir and the persistent challenge of HIV eradication: Biological barriers, therapeutic innovation, and future research directions
- Medivault: standardized storage system for medication safety in inpatient wards – A kaizen-based quality improvement initiative
- The Gateway to Quality Care: Evidence-Based Initial Patient Assessment
- Ultra-rapid thrombolysis in 19 minutes: Breaking conventional door-to-needle benchmarks
- Distinguished Alumni: A journey rooted in Kauvery
- Journal Scan: A review of images in clinical medicine of immediate clinical significance, harvested from major international journals
- Editorial
- Prolonged cardiac arrest during primary PCI in acute anterior wall myocardial infarction
- ASD with Partial Anomalous Pulmonary Venous Connection (PAPVC)
- Quality Improvement to improve patient safety and satisfaction: Effective whiteboard communication tool.
- A comparative study on dysphagia management & optimization of nutritional status among acute stroke patients
- Clinical case study on management of glycemic variability in gestational diabetes mellitus, diet as a primary therapeutic tool
- A rare case of multiple large bowel perforations following air blast injury through the rectum
- Carcinoma of the lower esophagus managed by video-assisted thoracoscopic esophagectomy
- A tale of two twins: A detailed case presentation of preterm neonates with divergent clinical courses
- From fragile lines to fortified care: A nursing-led revolution in iv dwell time at Kauvery hospitals
- Navigating the two-stage elephant trunk procedure (CET): A nursing case study on postoperative vigilance and multidisciplinary care
- The 3C initiative: weaving a stronger fabric of care through monthly connection at Kauvery hospital Vadapalani
- ACL reconstruction rehabilitation in an adolescent athlete: A case report
- Myasthenia gravis
- Comprehensive care for Preterm & Low birth weight babies
- National Cardiac Life Support (NCLS) workshop at Kauvery Hospital
- Strengthening institutional commitment to patient safety: Report on a structured training workshop at Kauvery hospital
- Dietary management for the RTA with polytrauma
- Successful staged Percutaneous Coronary Intervention (PCI) in a patient with cardiogenic shock and triple vessel disease
- Early infantile developmental epileptic encephalopathy
- Peutz Jeghers Syndrome
- Emergency nursing management of a patient with? Meningitis and spinal abscess
- Report on continuing nursing education (CNE) program
- Dual lipid-lowering therapy: Maximizing IDL-C reduction through complementary mechanisms
- Calvarial Osteomyelitis & CSF Leak Management Post Pituitary Surgery
- Journal Scan
- என் செவிலிய பணி
- Editorial
- Diffuse axonal injury grade III
- Cerebral venous thrombosis
- Arrhythmogenic right ventricular cardiomyopathy presenting with sustained ventricular tachycardia in an adolescent male: A case report
- Imaging the Invisible: Paediatric Venous Malformation of the Ankle with DSA Confirmation
- Clinical pharmacy perspective: Can antiplatelet therapy be used for preventing thrombus formation in the left atrium and apical clot?
- Left carotid endarterectomy with coronary artery bypass grafting (CABG)
- Left pulmonary artery stent restenosis in a patient with repaired tetralogy of fallot
- Preventing the preventable: Clinical pharmacy role in managing severe hypoglycemia in an elderly patient on glimepride
- Severe aortic regurgitation with ascending aortic dilatation in a young adult with bicuspid aortic valve
- A Case Study on Surgical Repair of Subclavian Artery Aneurysm.
- Thoracoabdominal and suprarenal Abdominal Aortic Aneurysm: Surgical and Critical Care Management
- Heart to heart illness for mother and daughter
- Clinical Pharmacy of Torsemide: Toxicity and Safety Considerations in Elderly Patients – With an Embedded Case Report
- Tetanus with Autonomic Dysfunction in an Elderly Diabetic Patient with Restrictive Cardiomyopathy and Implanted Pacemaker: A Fatal Outcome
- Case study on MODY (Maturity onset diabetes of the young) – Taper down of the sulfonylurea doses
- Effectiveness of cryo-compression therapy in preoperative and postoperative orthopaedic patients: A case study
- Emergency laparotomy in a patient with bleeding duodenal ulcer
- Successful management of severe pre -eclampsia complicated by massive proteinuria and fetal growth restriction in a primigravida
- Blunt thoracoabdominal trauma with rib fractures and muscle laceration: A case report
- Flash fire injuries: A preventable catastrophe
- The River Within: A Journey of Life and Renal Care
- Evidence based management of cervical insufficiency
- Treacher Collin’s Syndrome
- Effective nursing triage and stroke code activation in acute hypertensive intracerebral haemorrhage presenting with sudden loss of consciousness
- Euglycemic Diabetic Ketoacidosis: A Diagnostic Challenge in Clinical Practice
- IV – Nurse Day Celebration-2026
- Nutritional management in deceased donor liver transplantation: A case study of decompensated chronic liver disease with hepatocellular carcinoma
- The body’s sudden shutdown: Vasovagal syncope
- Weaning from Ryle’s Tube Feeding to Oral Diabetes Diet in a patient with Diabetes, and with Respiratory Compromise
- Successful management of traumatic lung injury using veno-venous ECMO in a young RTA patient
- Cne certification program on prevention and management of venous thromboembolism (VTE): Risk assessment, early recognition, prevention, and evidence-based management
- Nurses day celebration 2026: A week of recognition, learning, and empowerment
- Electrical shock and its management
- Diagnostic approach to connective tissue disorder: Spotlight on adult-onset still’s disease
- Gastric varices in chronic liver disease managed with parto procedure
- Pararenal abdominal aortic aneurysm – preparation is the key to successful repair
- Journal Scan: A review of images in clinical medicine of immediate clinical significance, harvested from major international journals
- தாயும் சேயும்
